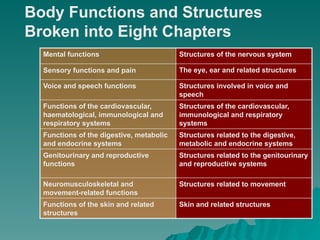
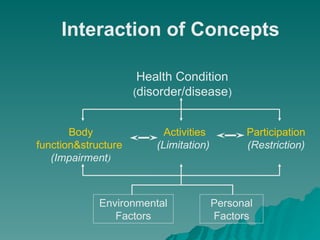
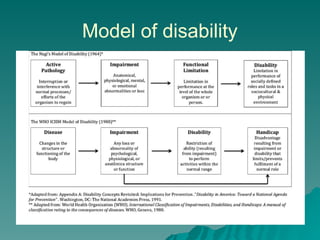
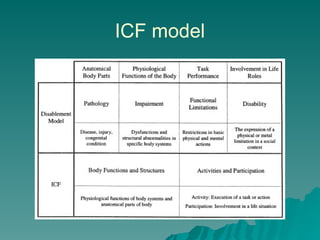
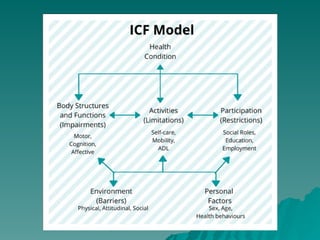
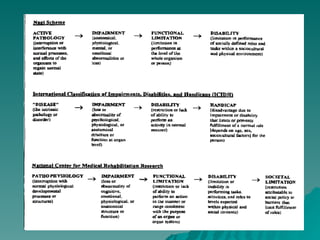
The document introduces the International Classification of Functioning, Disability, and Health (ICF), emphasizing its role in describing the impact of health conditions on human functioning and providing a common language for communication across health disciplines. It distinguishes 'disablement' as a global term reflecting various consequences of health issues on functioning and advocates for enabling environments in the workplace for individuals with disabilities. The ICF framework categorizes individual functioning into domains of body functions, activities, and participation, highlighting the interaction between health conditions, personal factors, and environmental influences.