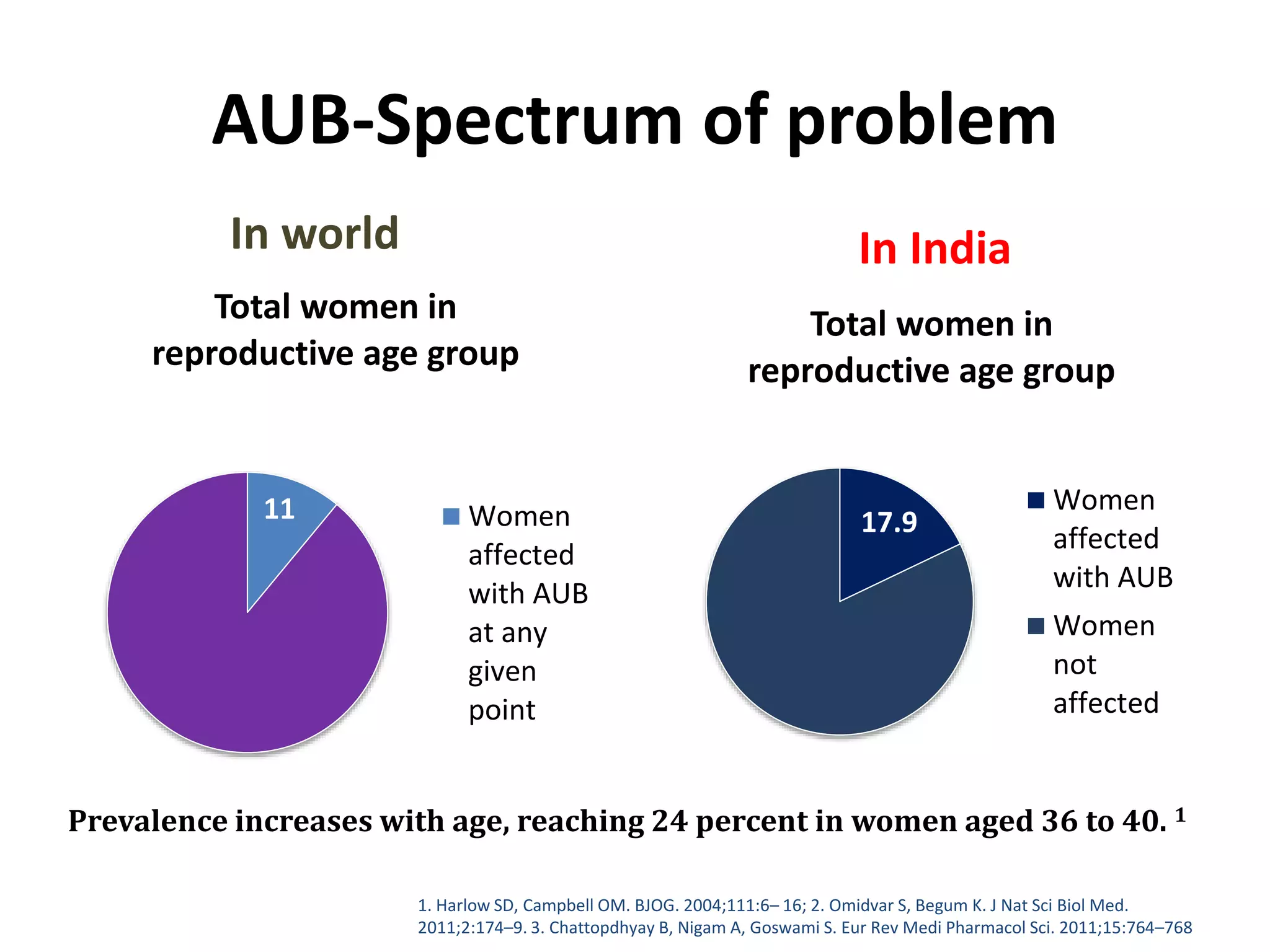
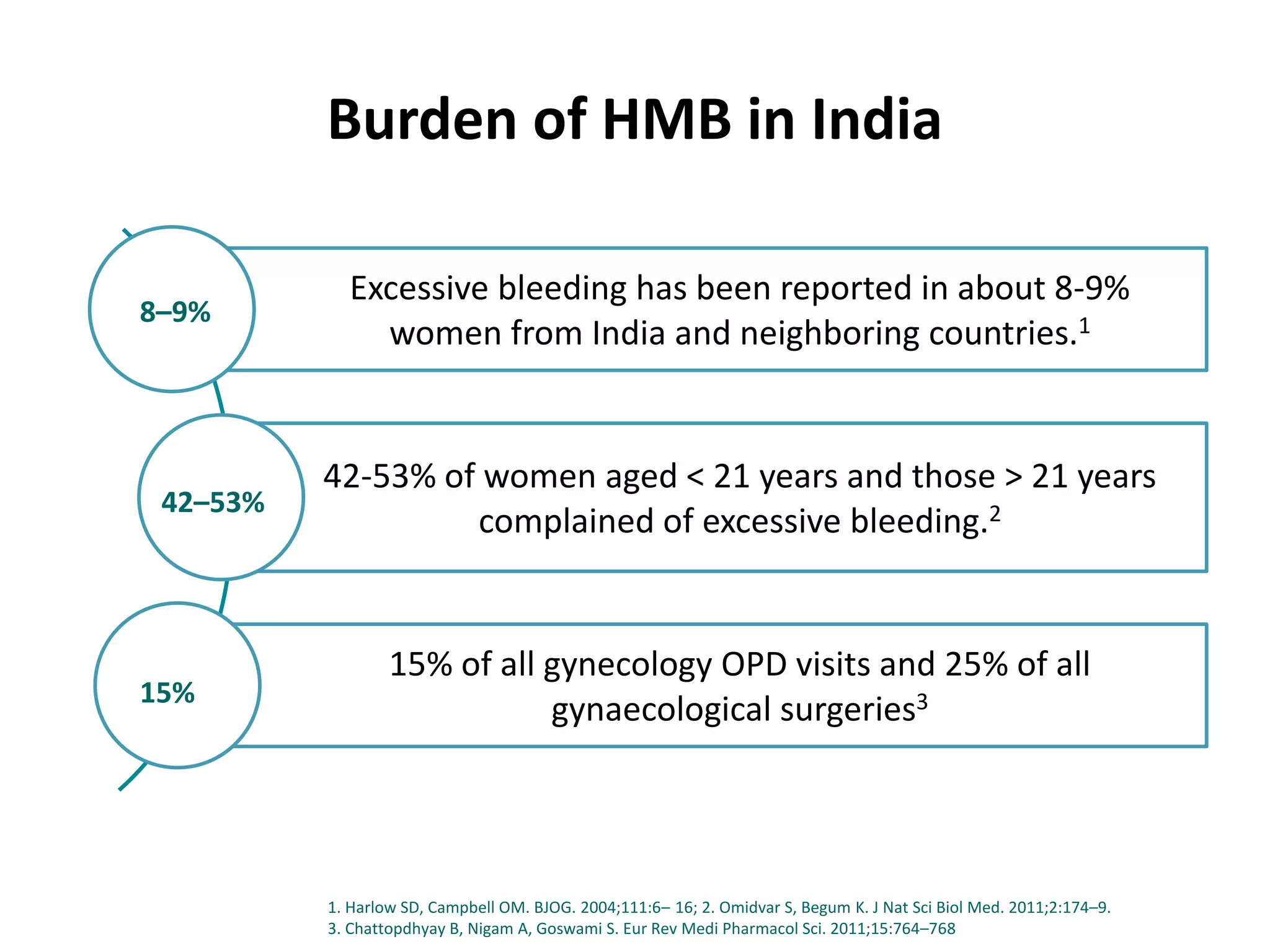
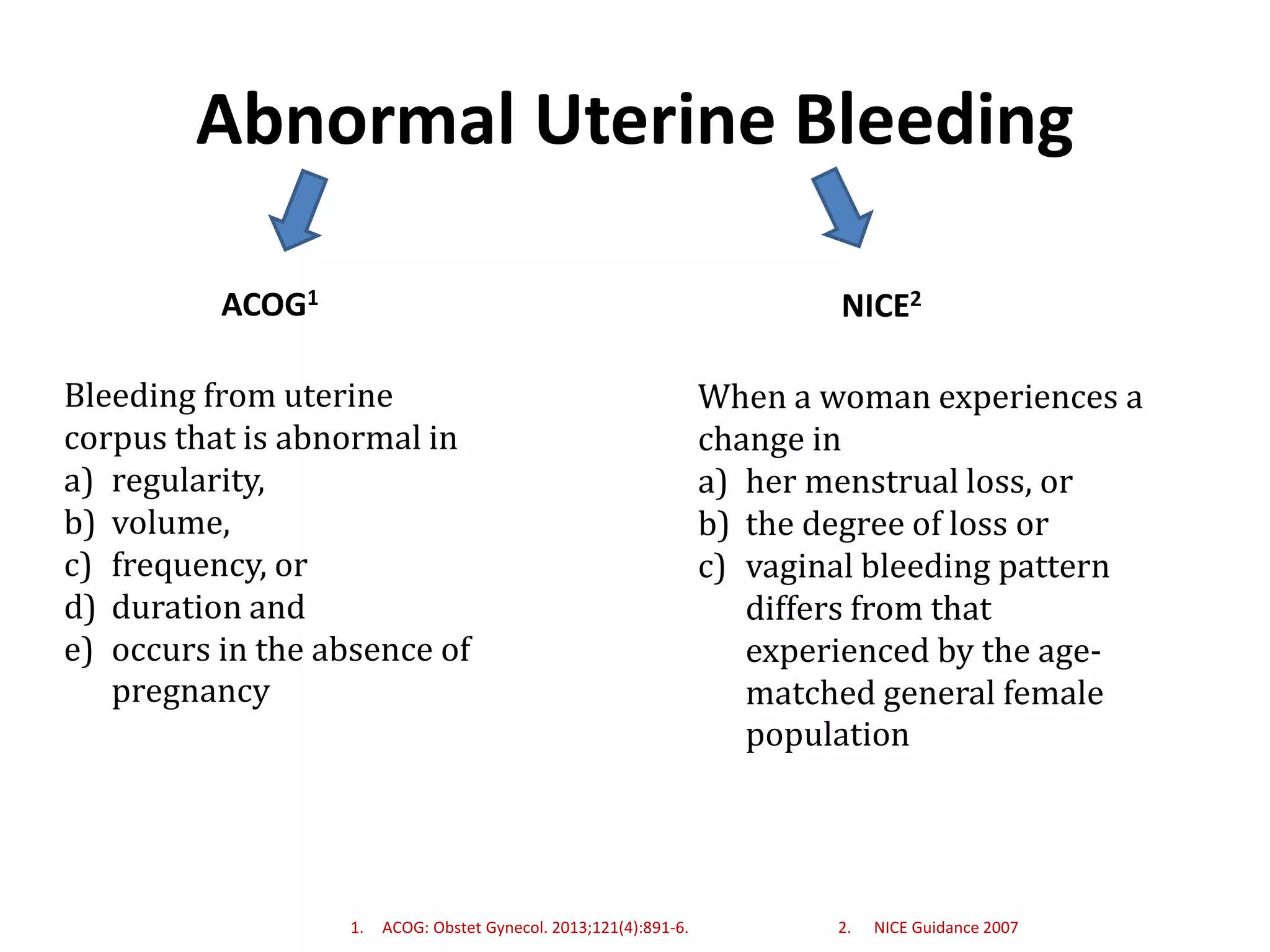
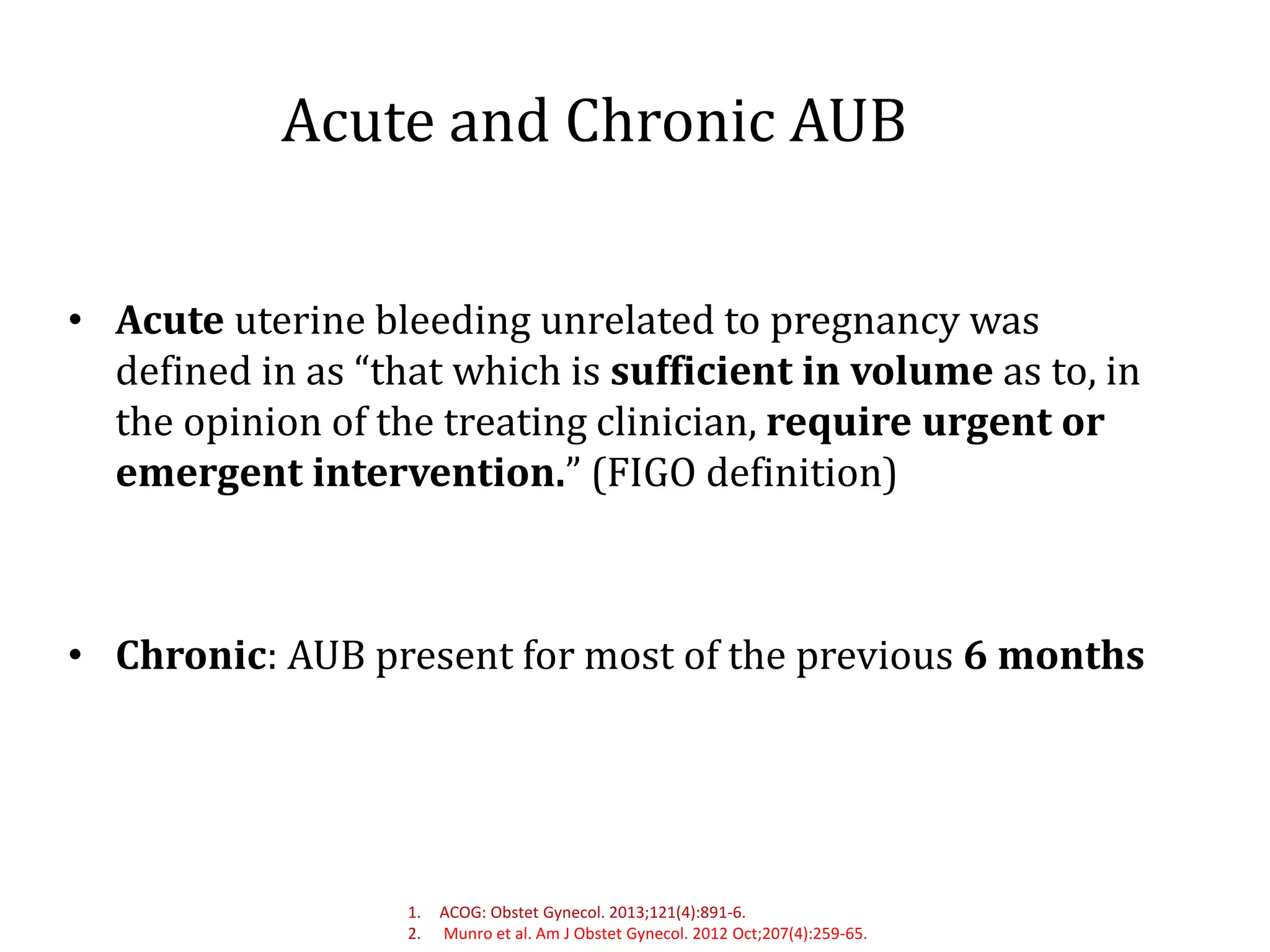
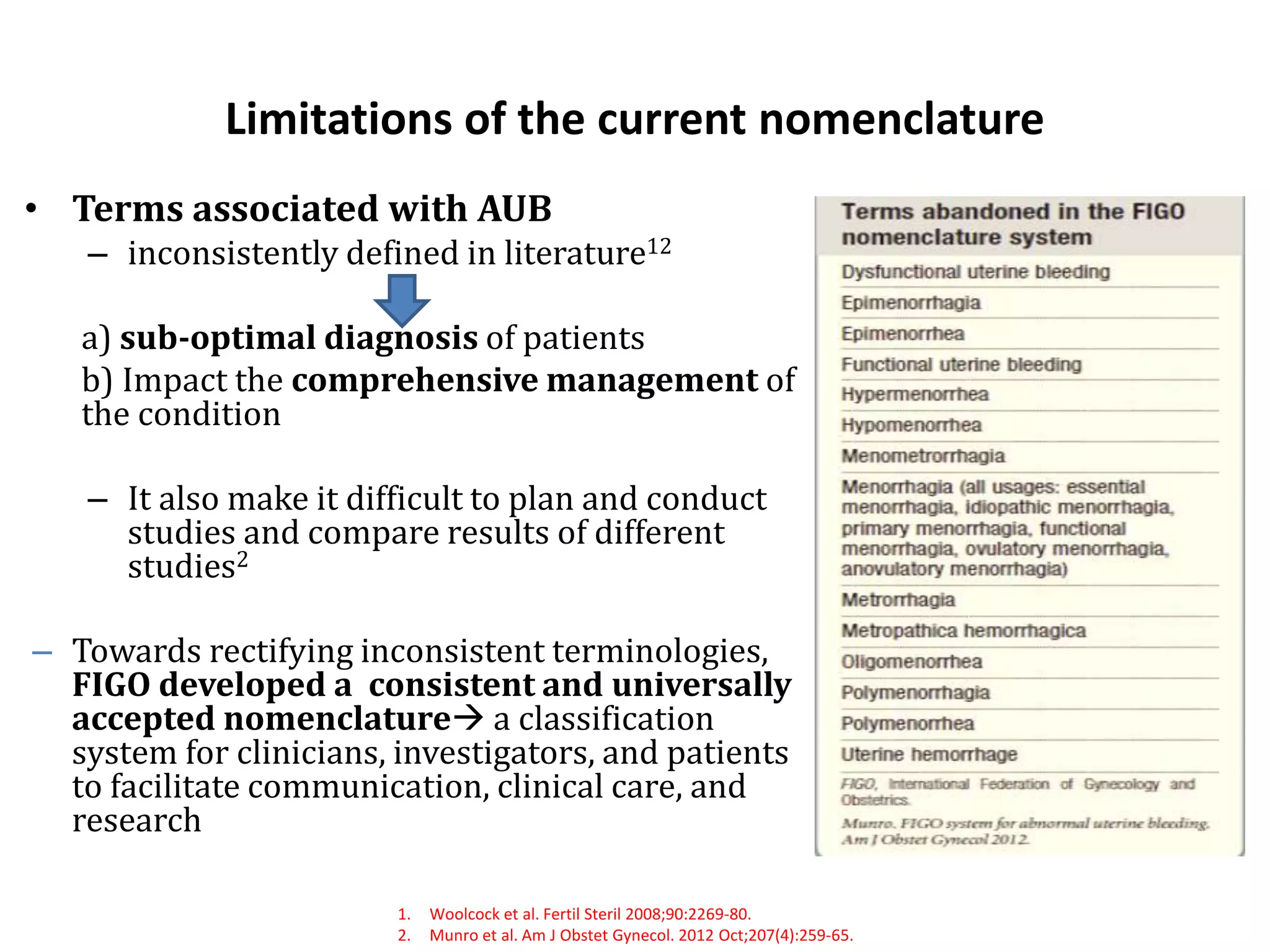
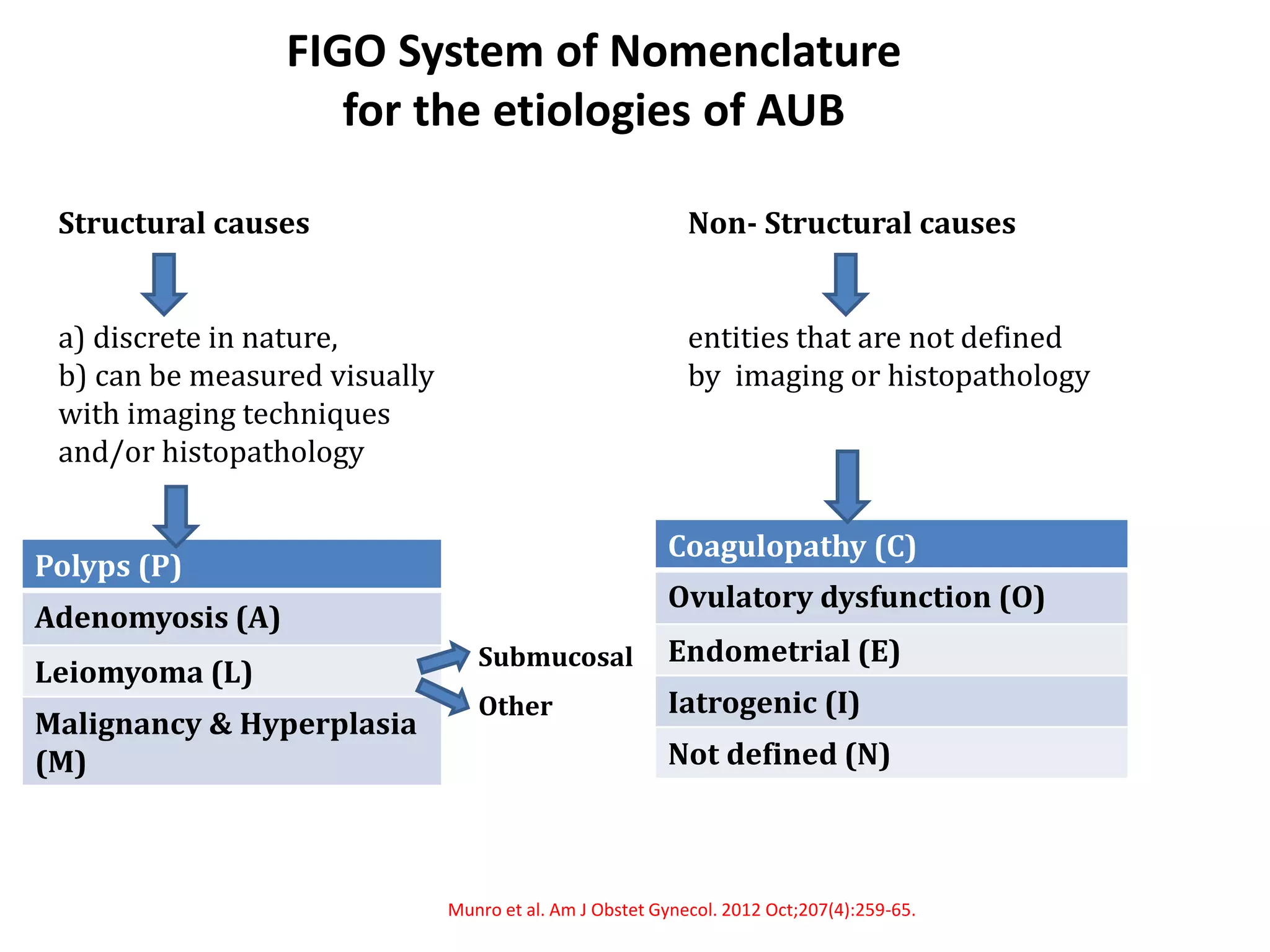
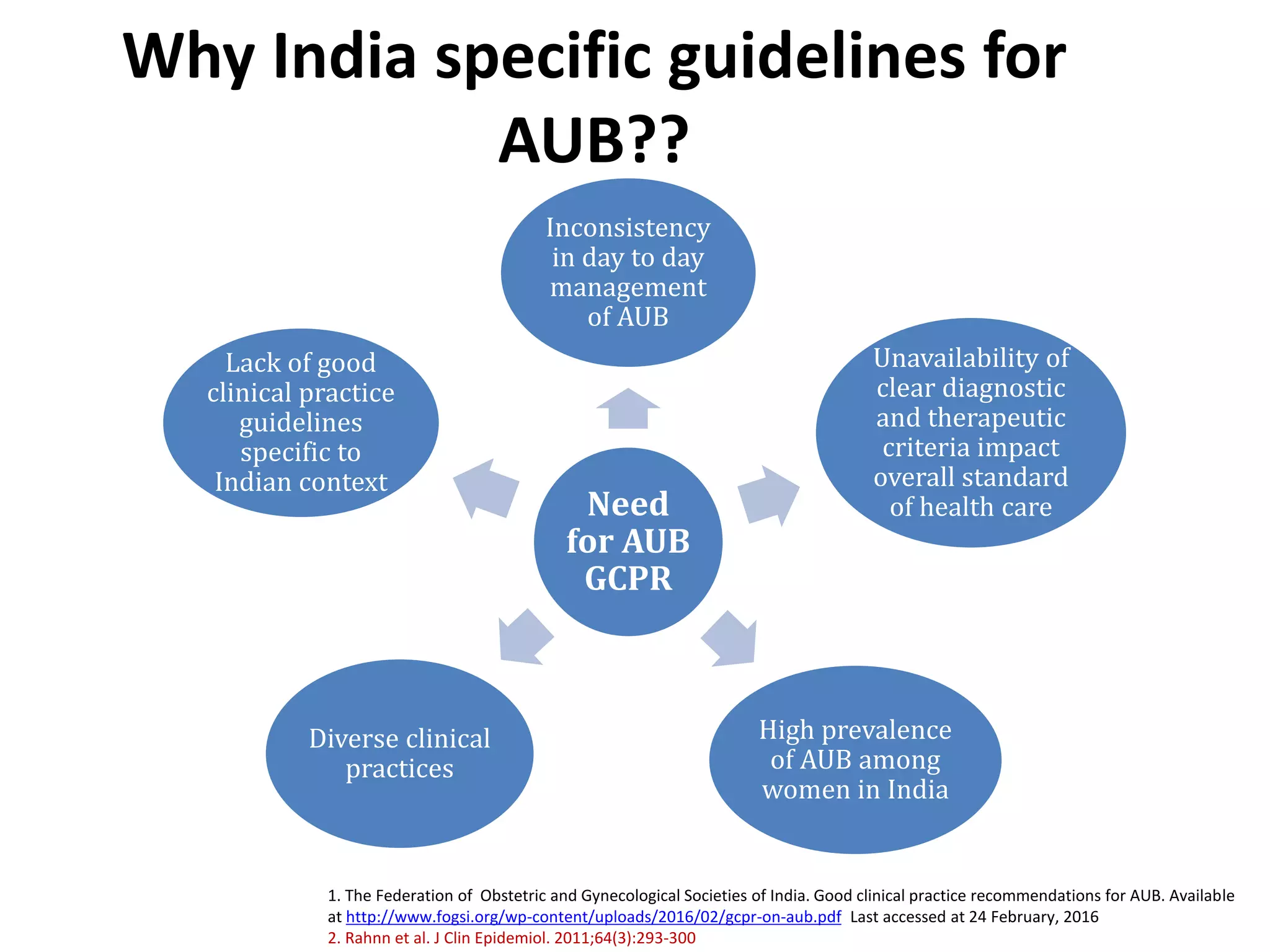
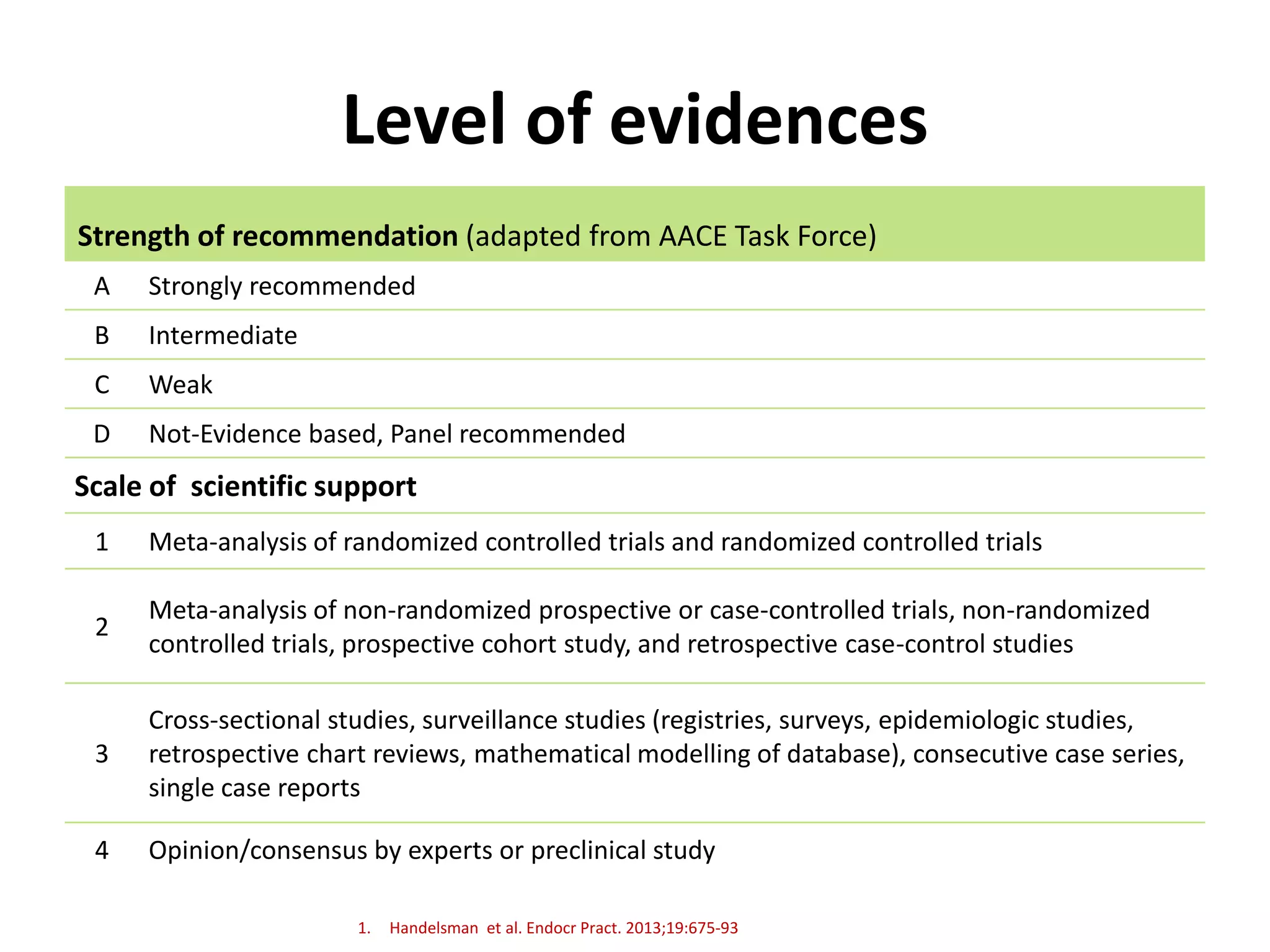
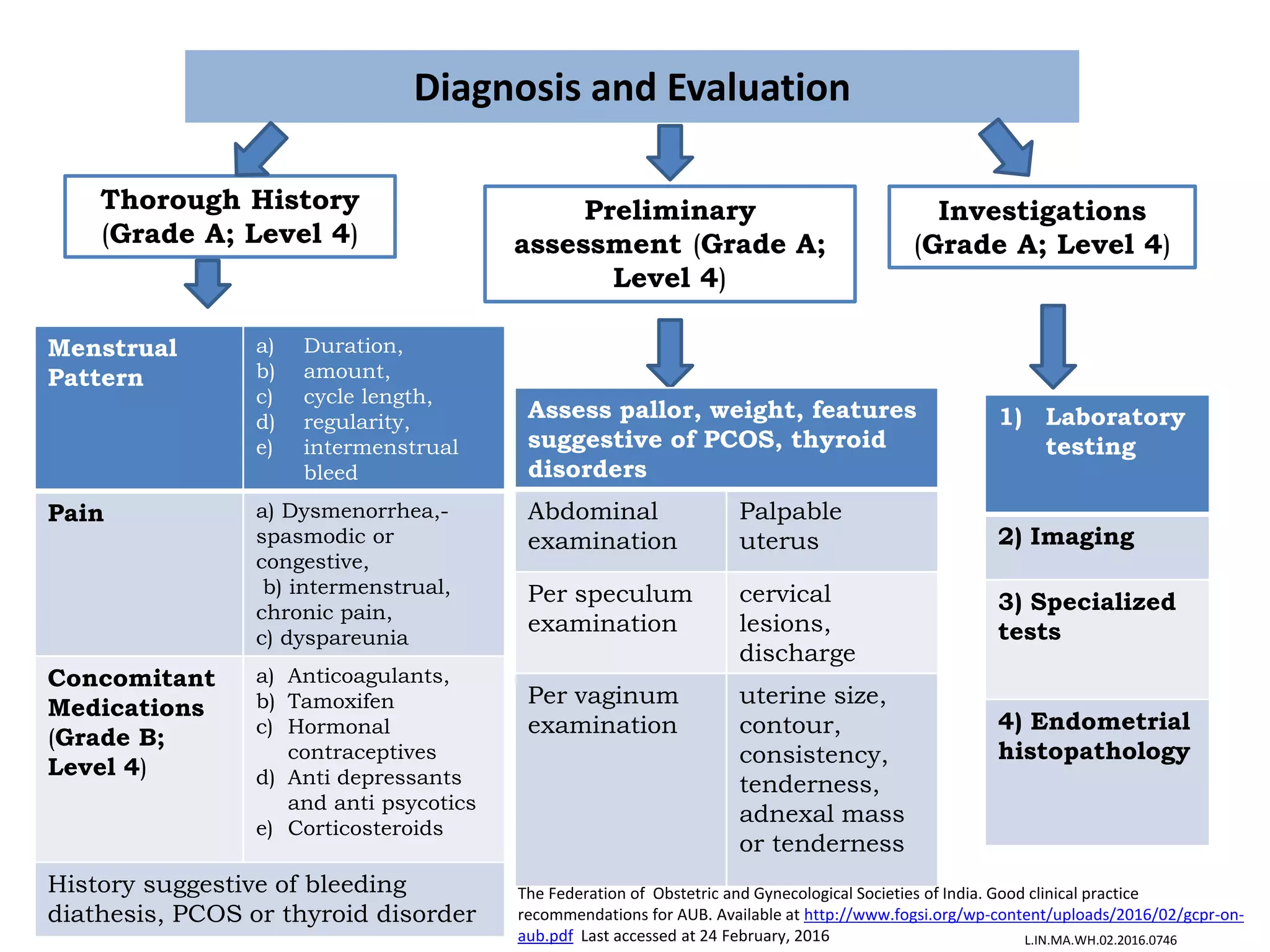
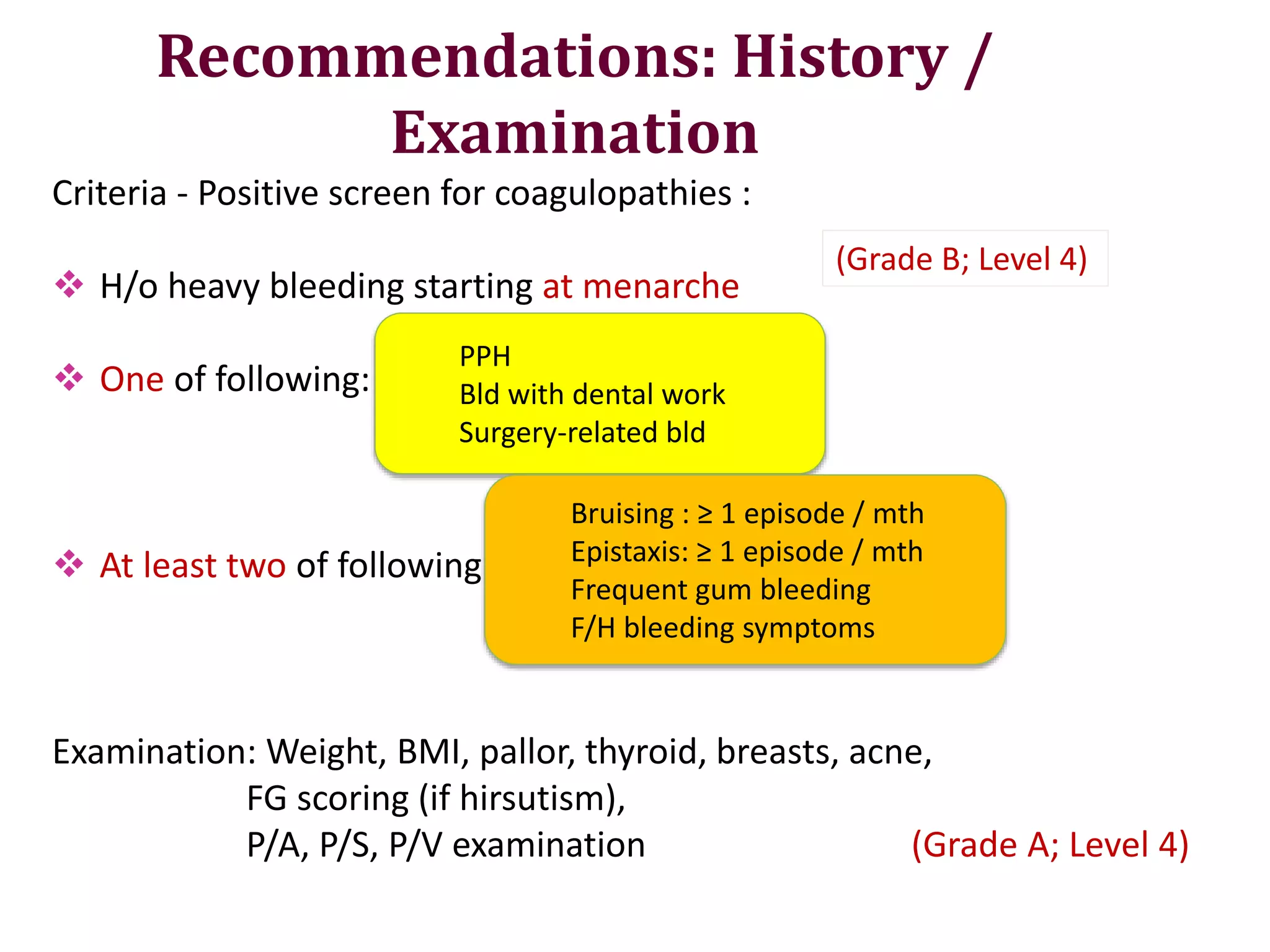
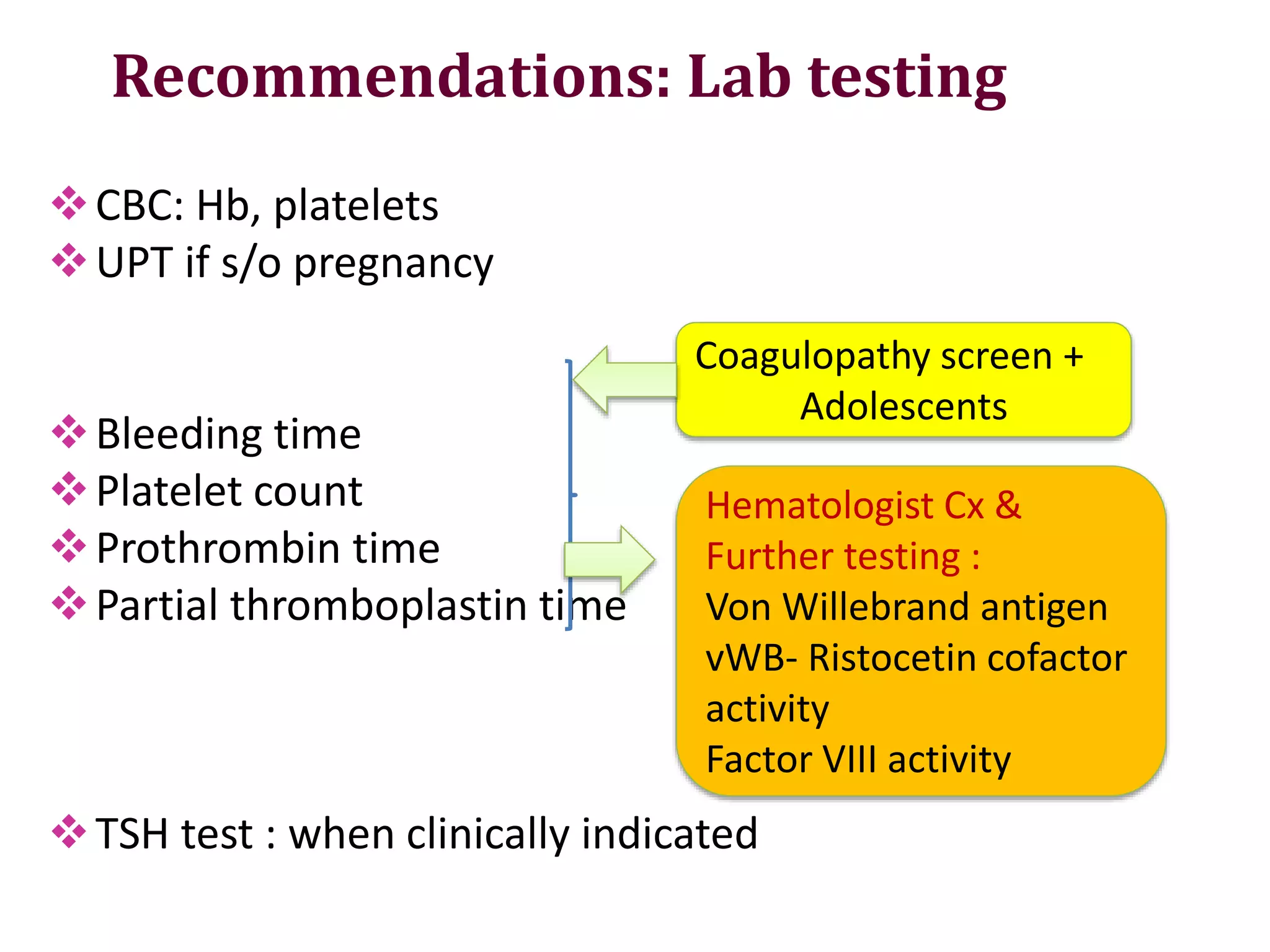
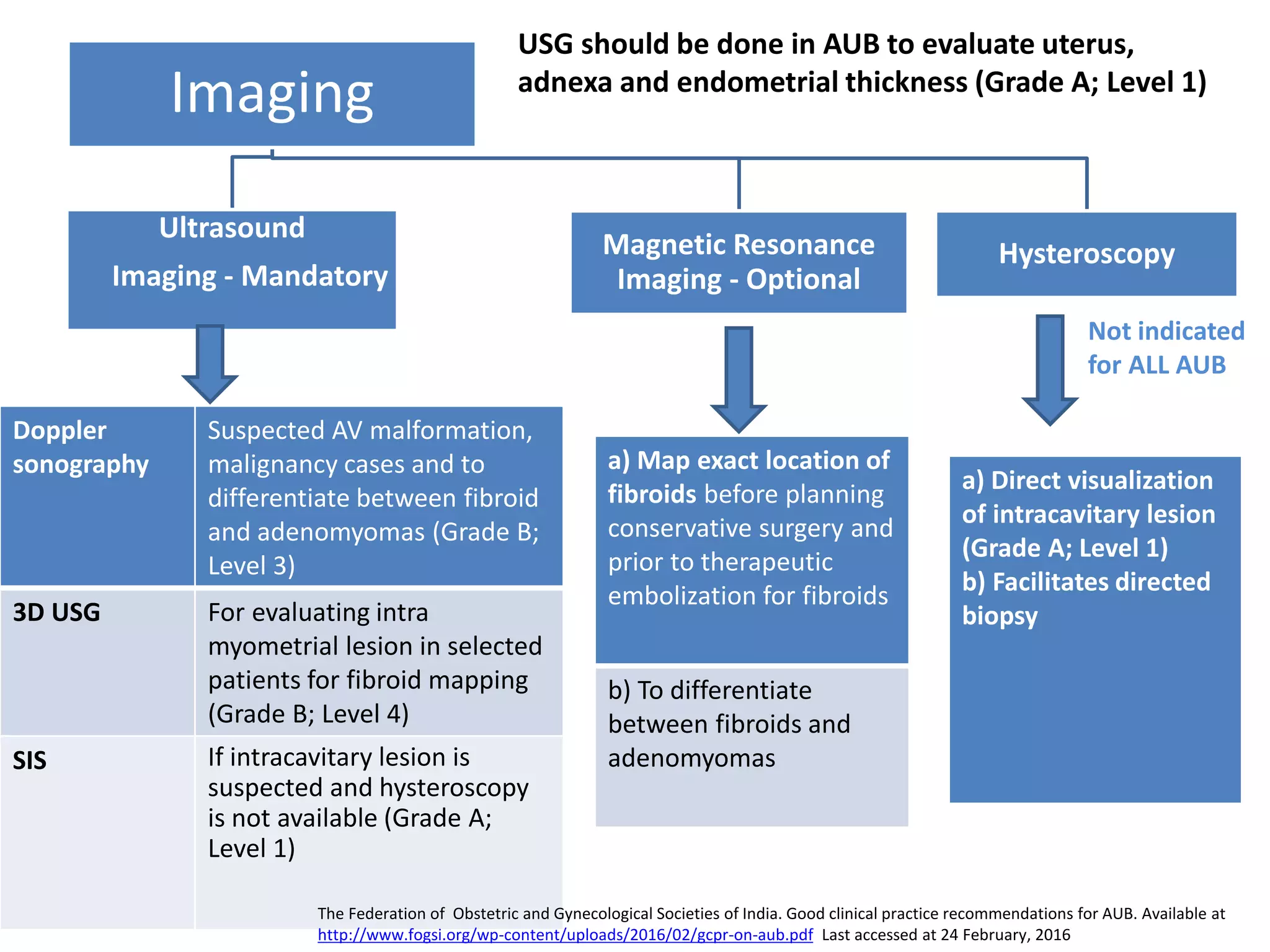
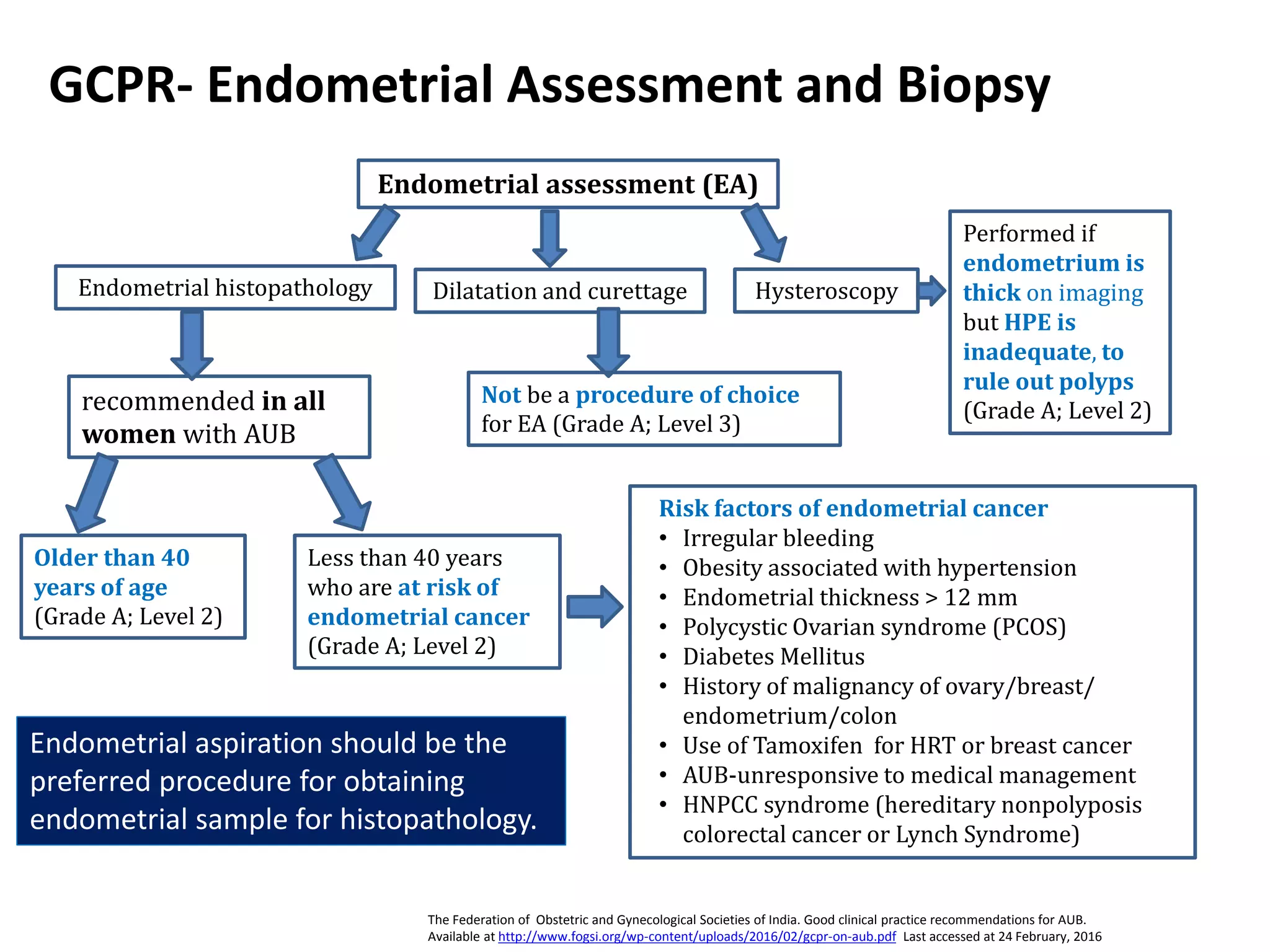
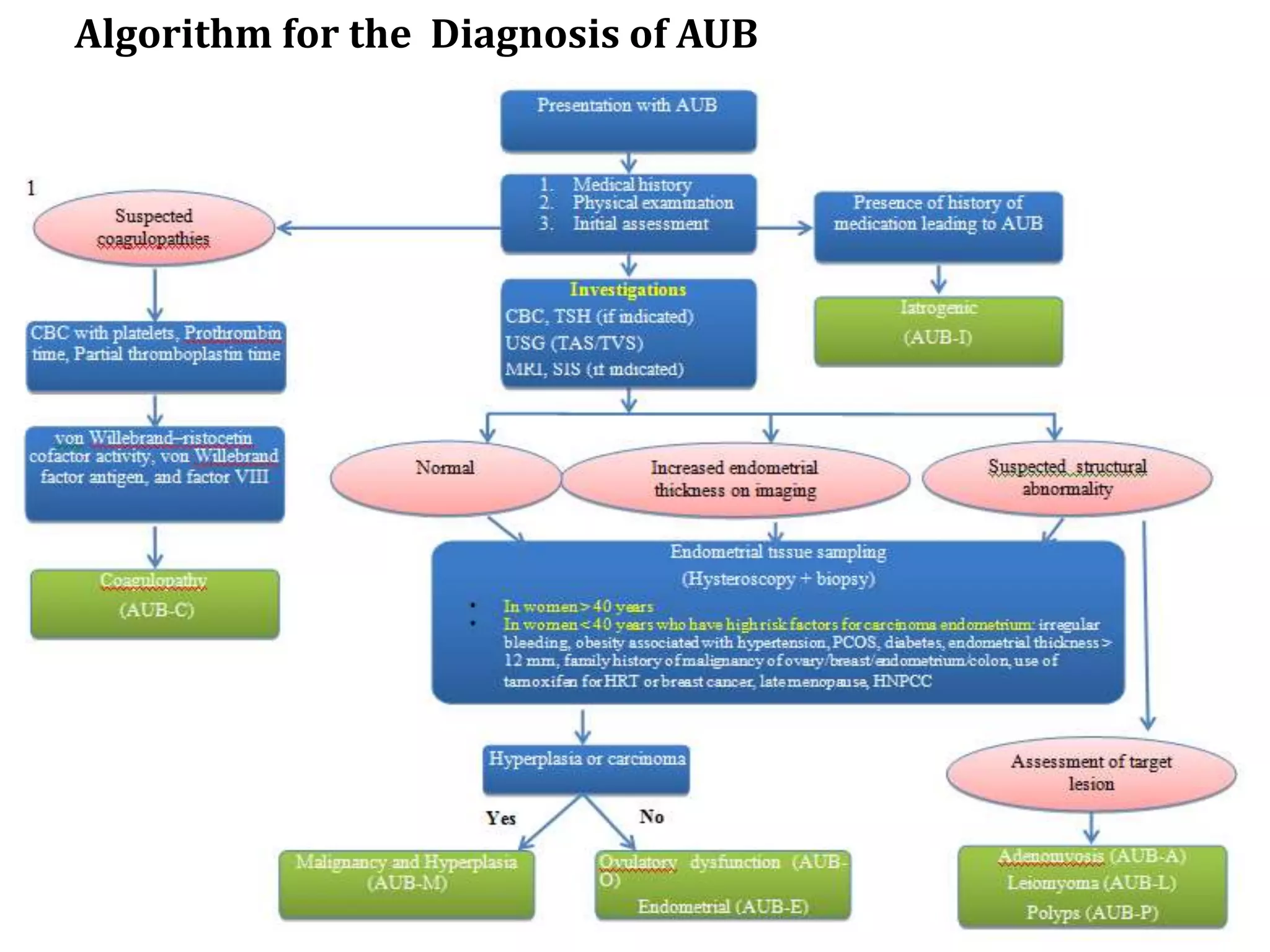
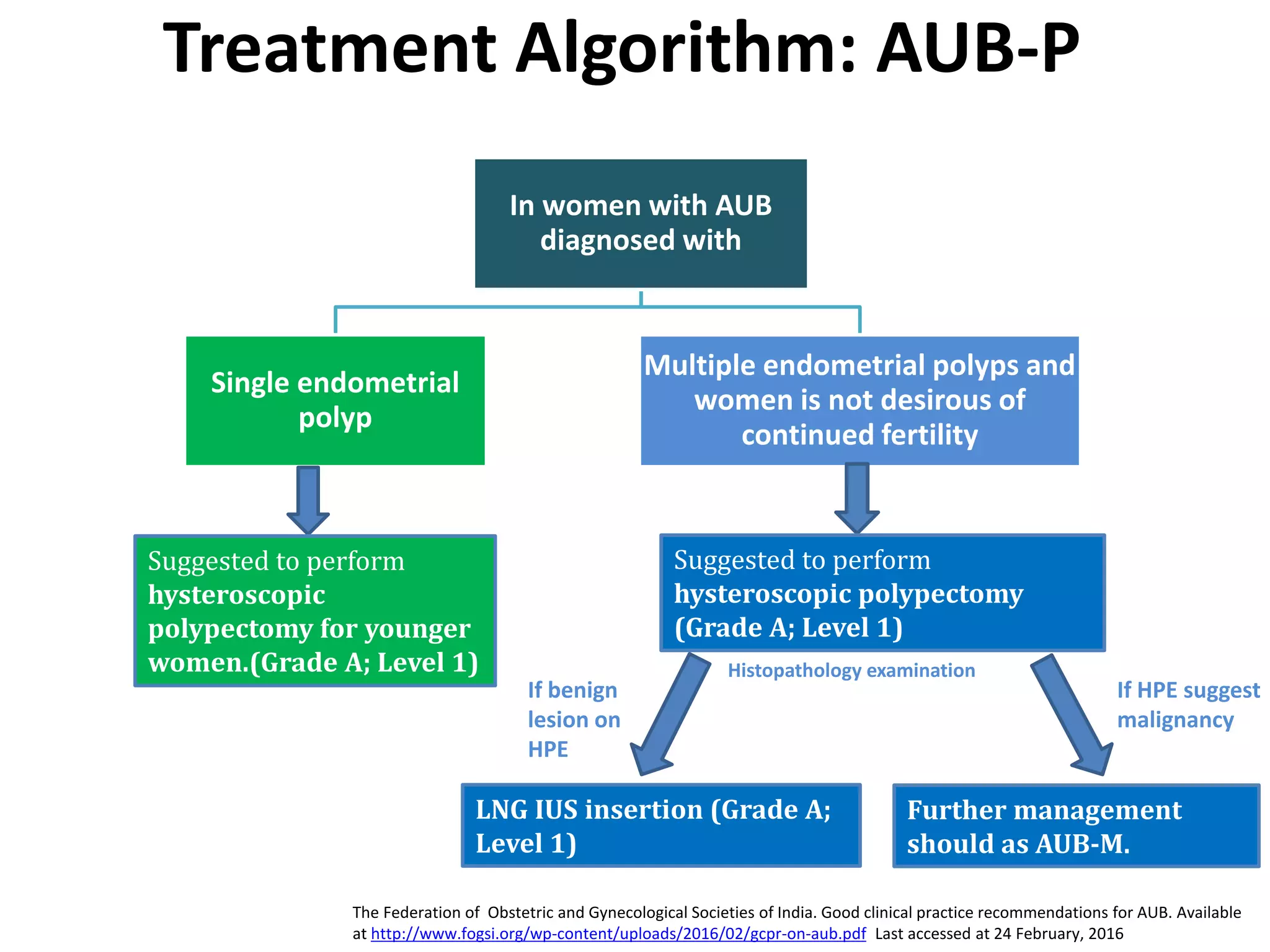
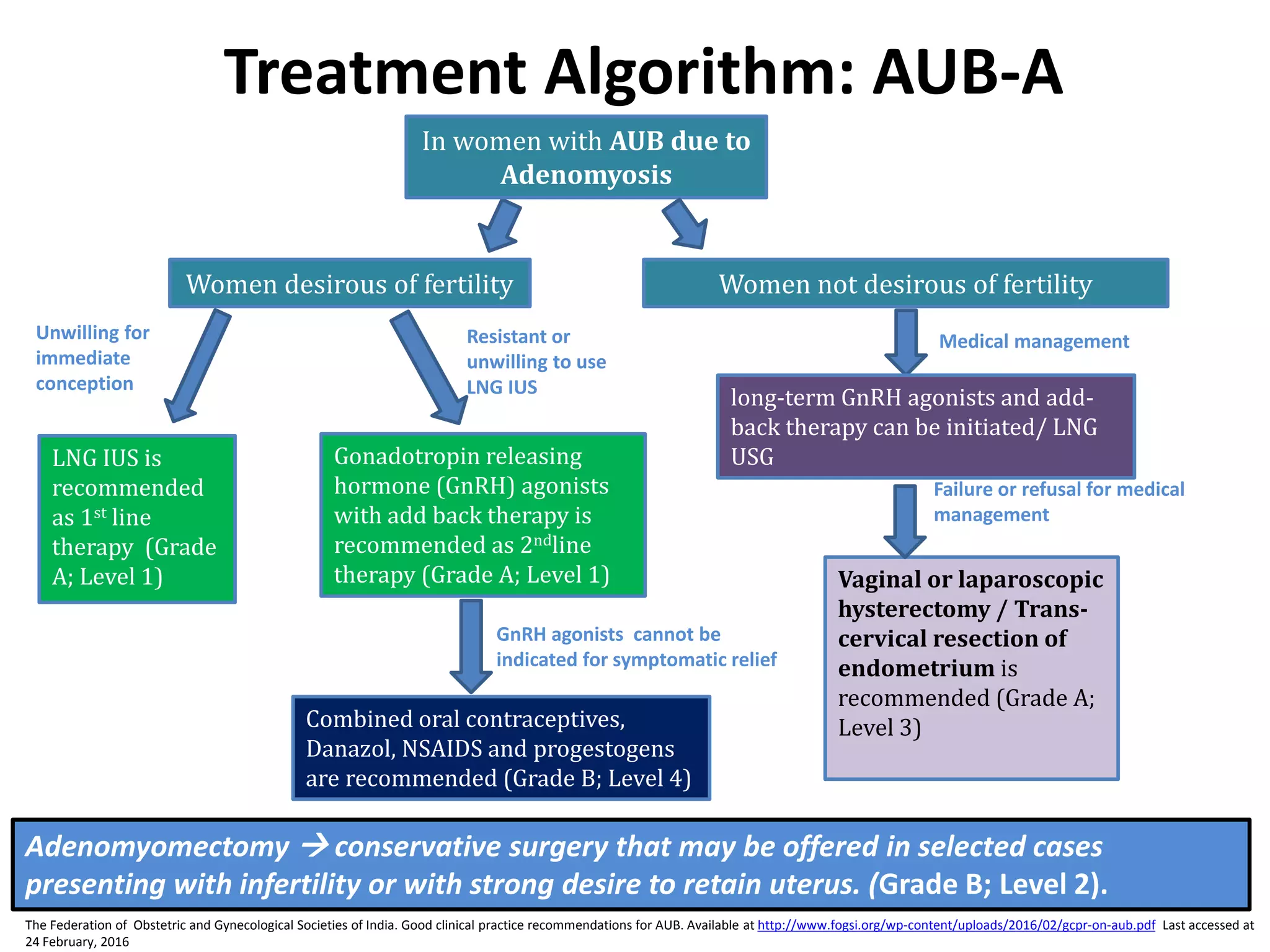
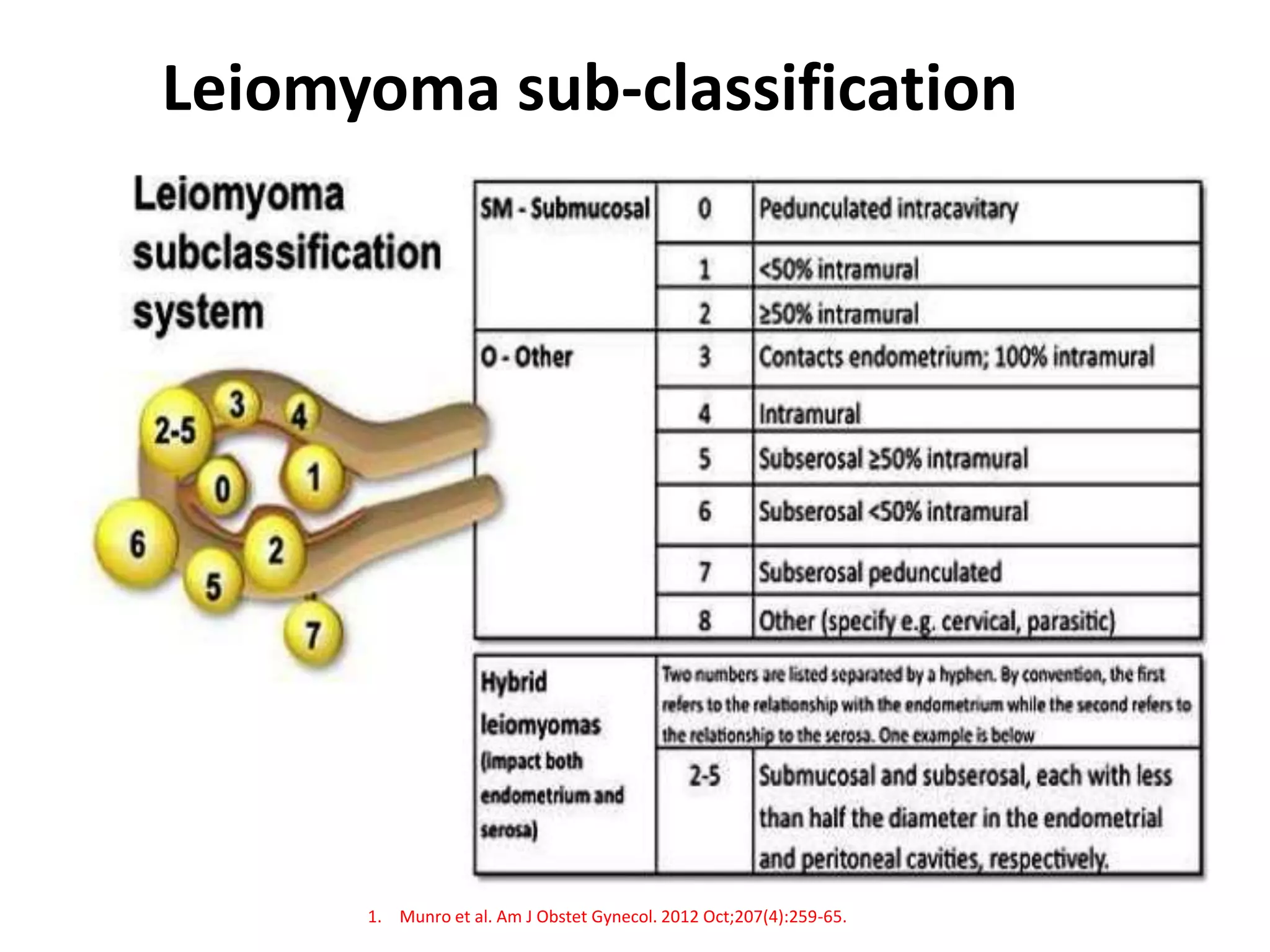
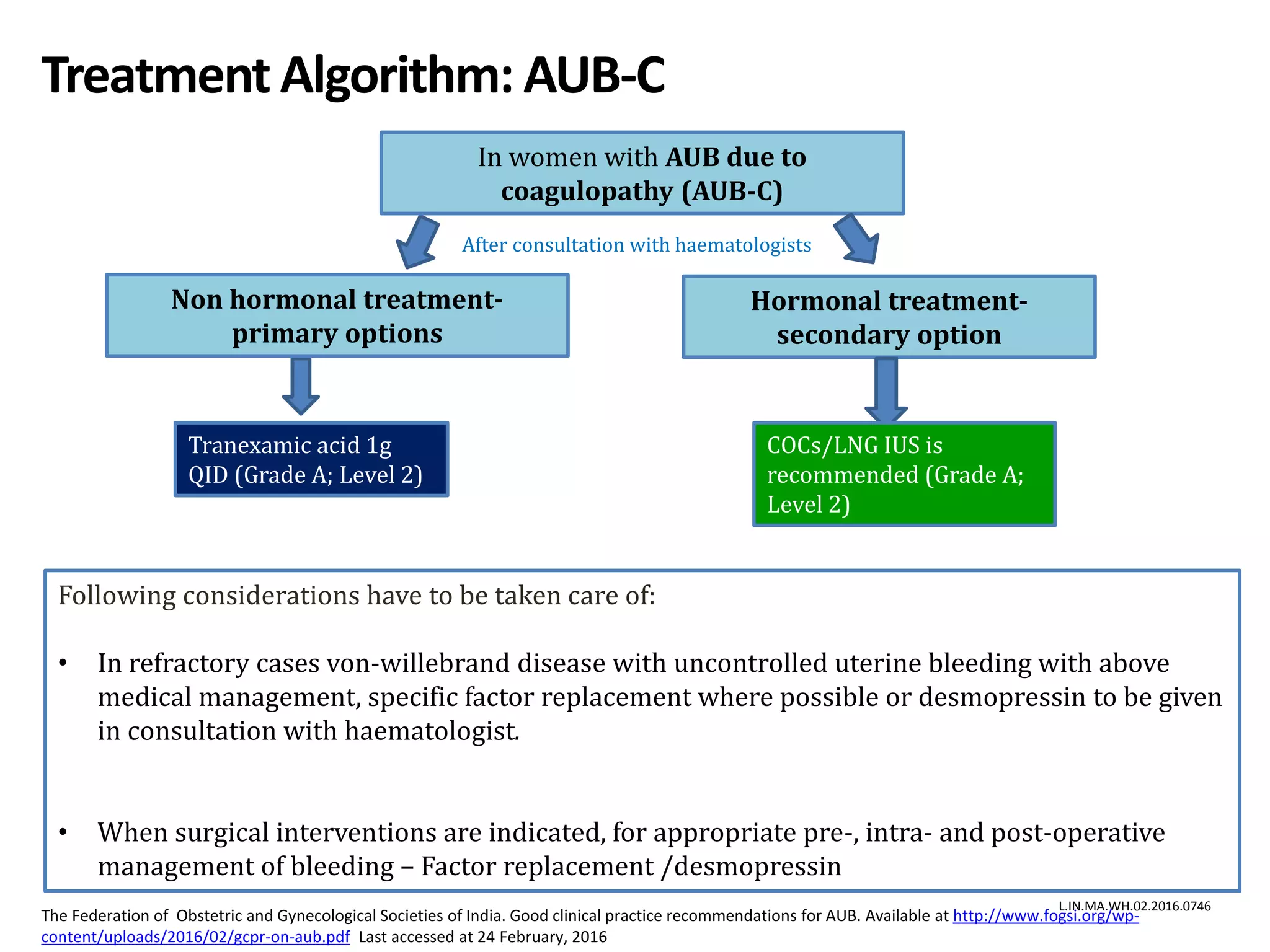
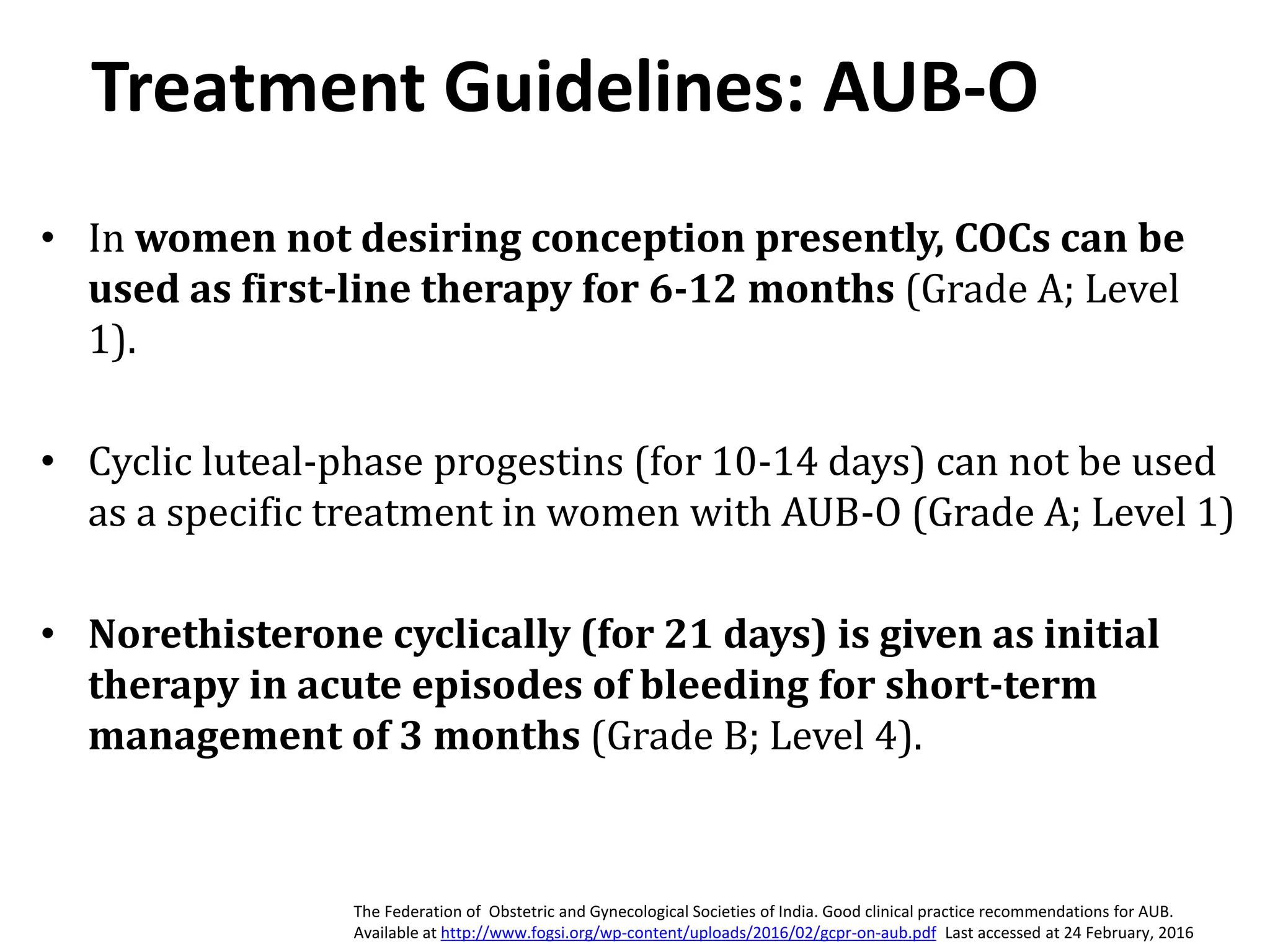
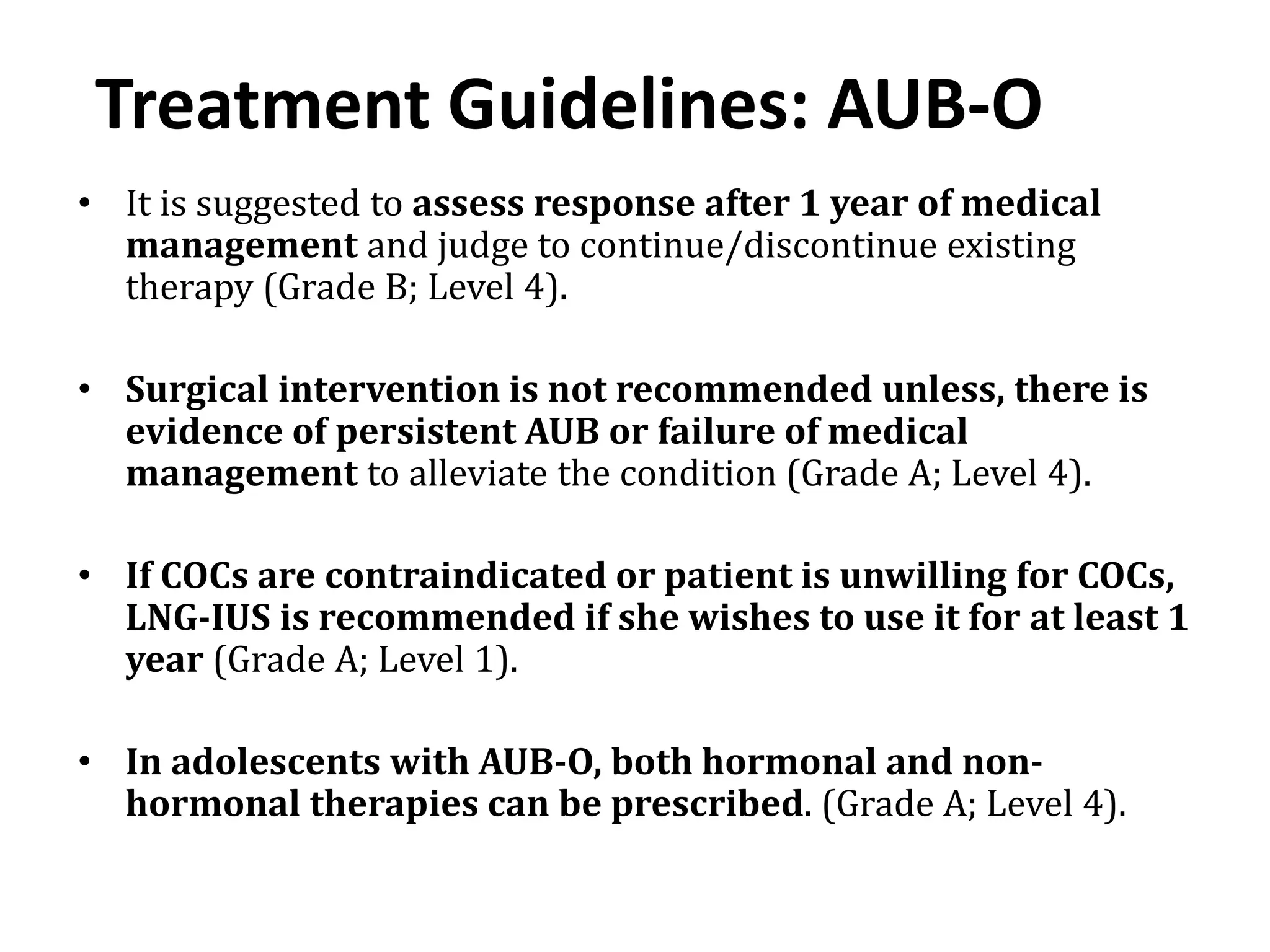
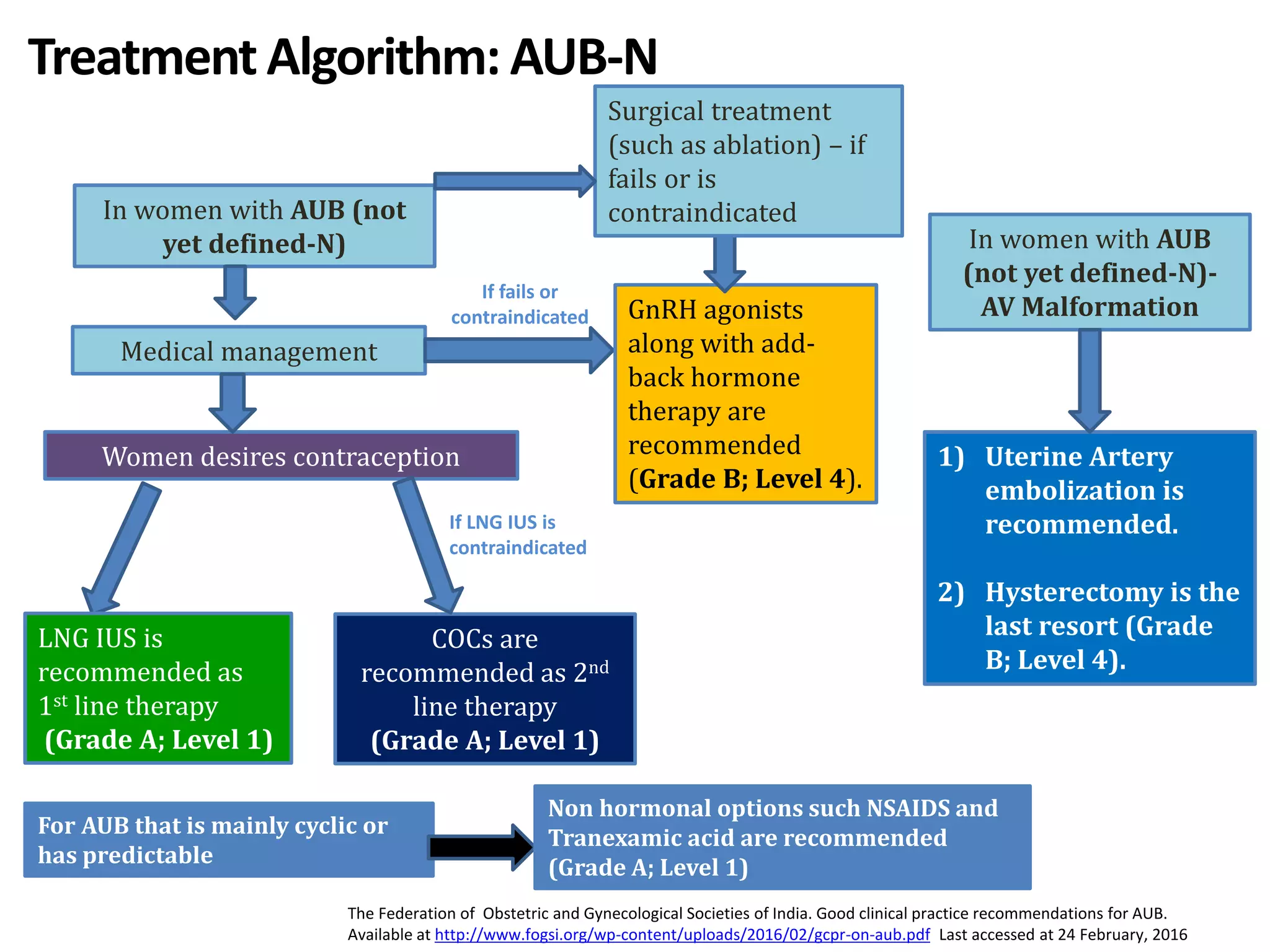
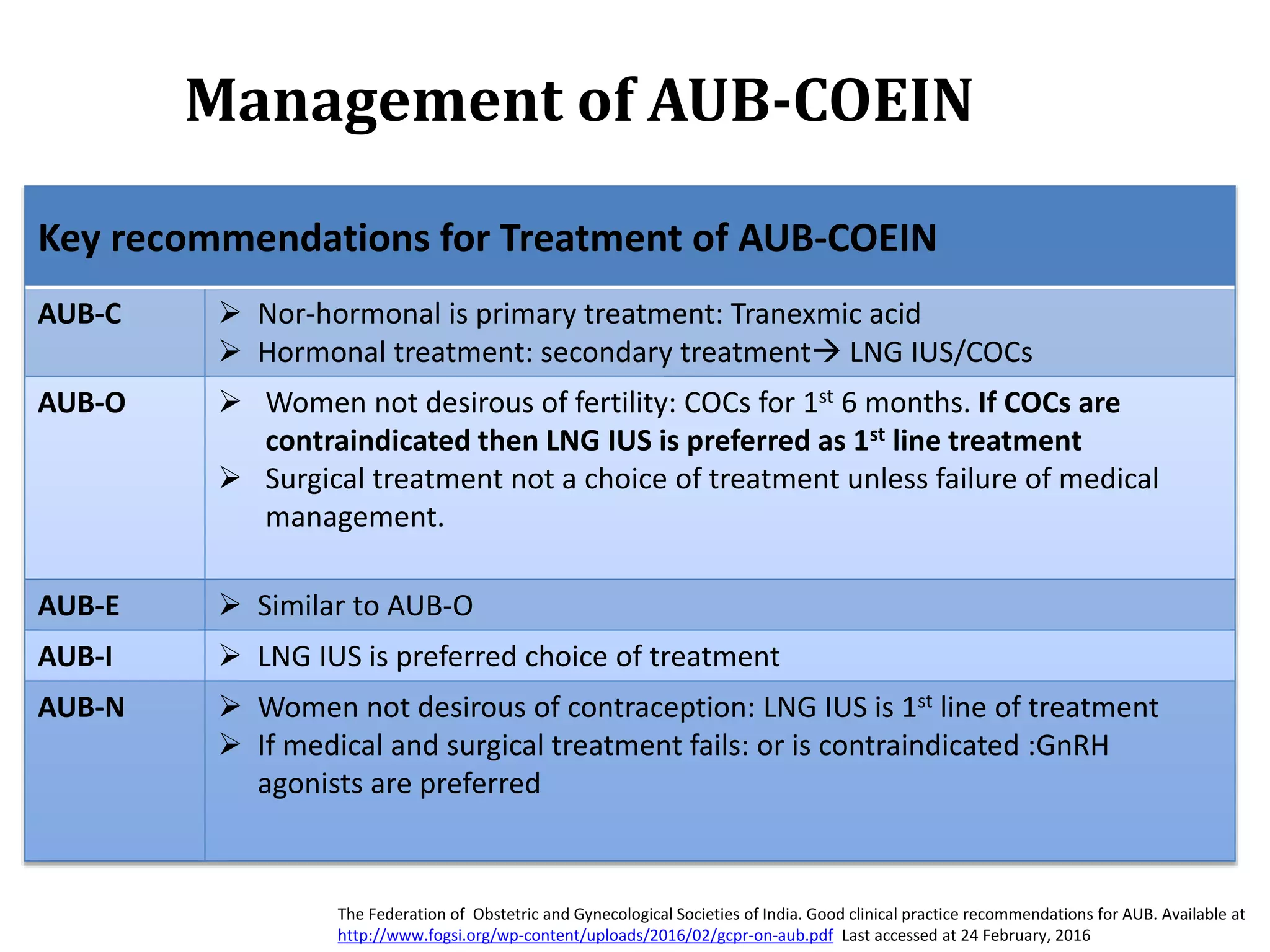
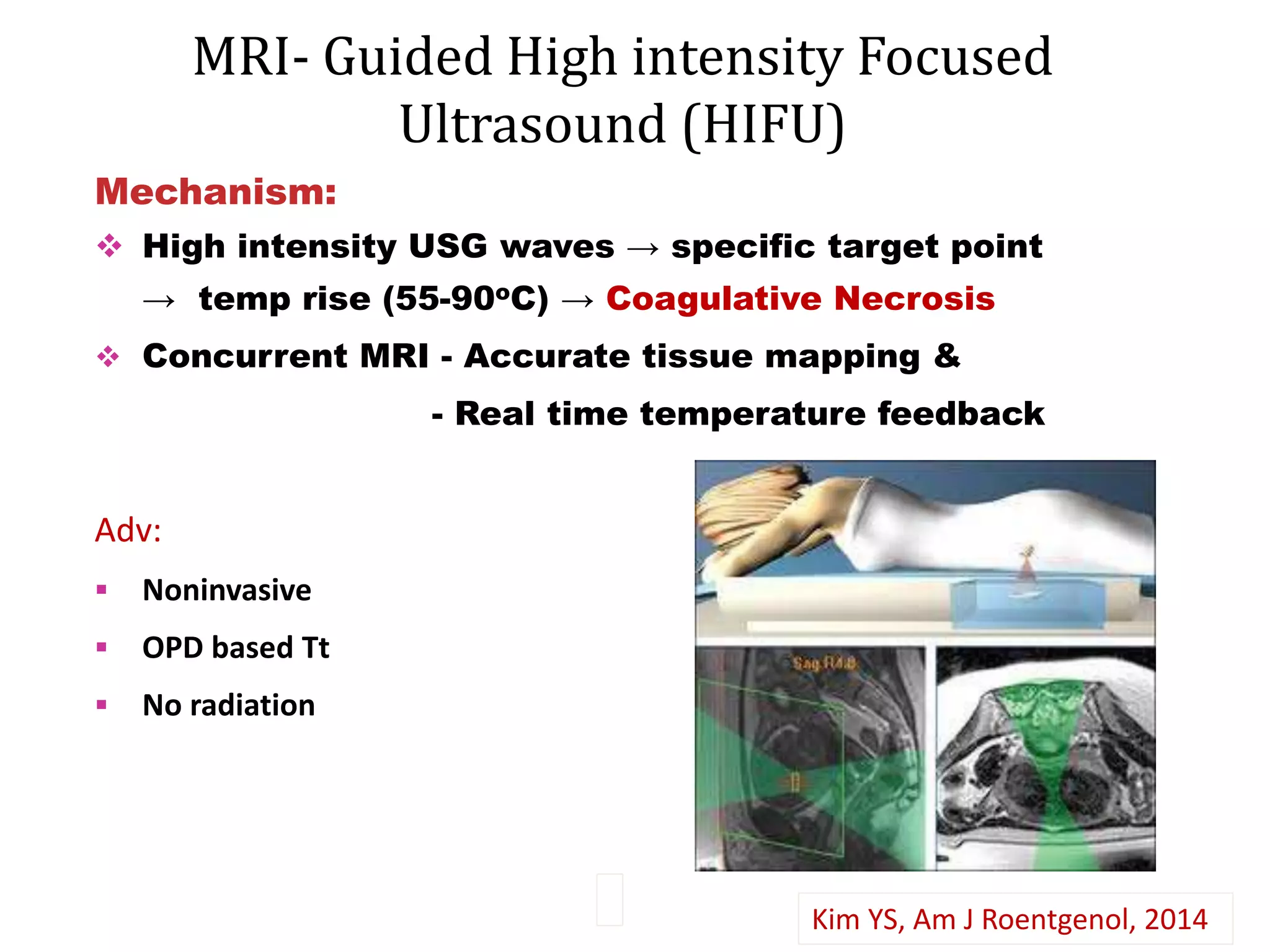
This document provides guidelines for evaluating and managing abnormal uterine bleeding (AUB) from an Indian perspective. It discusses the need for India-specific guidelines given the high prevalence of AUB in India and variability in clinical practices. The guidelines recommend using the FIGO PALM-COEIN classification system and provide algorithms for the diagnosis and management of AUB. Evaluation involves a thorough history, physical exam, and targeted investigations based on risk factors. Management algorithms are provided for the different structural and non-structural causes of AUB identified in the PALM-COEIN system from an evidence-based perspective in Indian women.



















































![ABNORMAL_UTERINE[1] DR SS NANda abnormal DA.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/abnormaluterine1drssnanda-250706172120-db732f7a-thumbnail.jpg?width=640&height=640&fit=bounds)

















































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)







