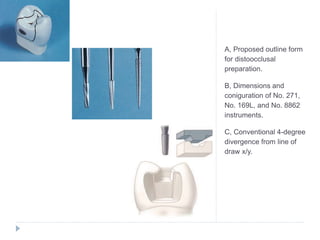
This document provides an overview of inlays and onlays. It defines inlays as restorations that involve the occlusal surface and one or more proximal surfaces of a posterior tooth, while onlays additionally involve restoring the cusp tips. The document discusses the indications, contraindications, classifications, advantages, disadvantages, tooth preparation process, and materials used for inlays and onlays. The goal of inlay and onlay preparations is to eliminate caries while maintaining adequate tooth structure for resistance and retention forms.



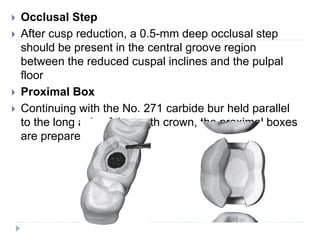







































![CAST_RESTORATIONS..................................[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/castrestorations1-251004081334-a7315aa9-thumbnail.jpg?width=640&height=640&fit=bounds)






























