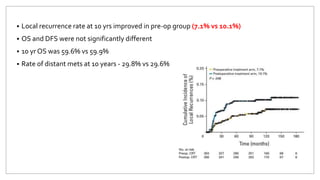
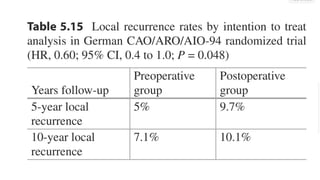
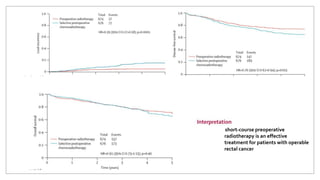
1) Short-course preoperative radiotherapy is an effective treatment for patients with operable rectal cancer, reducing the relative risk of local recurrence by 61% compared to selective postoperative chemoradiotherapy.
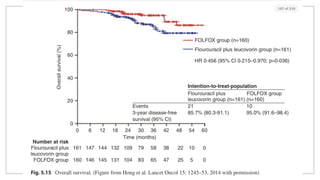
2) The addition of postoperative chemotherapy to preoperative chemoradiotherapy does not affect disease-free survival or overall survival in patients with stage T3 or T4 resectable rectal cancer.
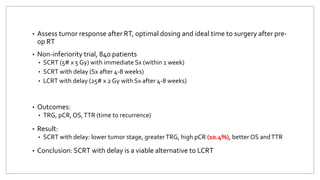
3) Short-course preoperative radiotherapy followed by delayed surgery results in lower tumor stage, greater tumor regression grade, and higher pathologic complete response rates compared to long-course radiotherapy followed by delayed surgery, with potential improvements in overall survival and time to recurrence.