











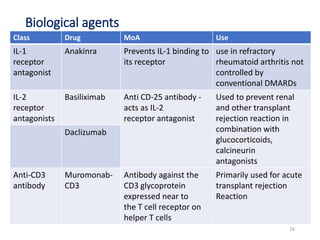



This document discusses immunosuppressant drugs, which inhibit immune responses and are used in organ transplantation and autoimmune diseases. It classifies major immunosuppressant classes including calcineurin inhibitors like cyclosporine and tacrolimus, mTOR inhibitors like sirolimus and everolimus, antiproliferative agents like azathioprine and methotrexate, glucocorticoids, and biological agents. For each drug class and examples, it explains mechanisms of action, therapeutic uses, and common adverse effects. The document provides detailed information on commonly used immunosuppressants to treat transplant rejection and autoimmune conditions.























































































