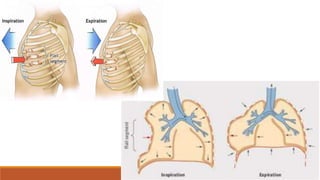
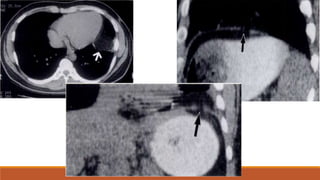
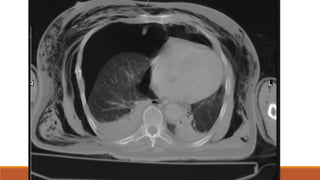
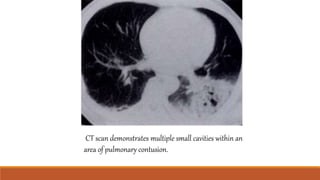
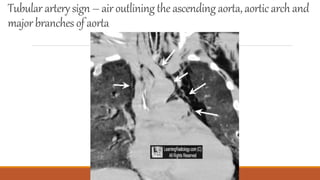
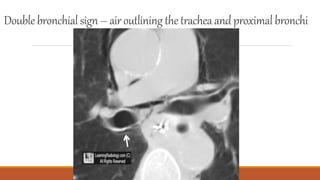
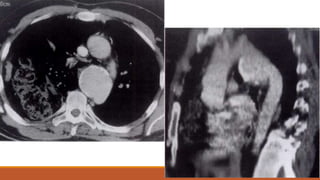
This document discusses chest trauma, including injuries to the thoracic cage, diaphragm, pleura, lungs, trachea/bronchi, mediastinum, and vascular structures. It outlines common causes of chest trauma like falls, blows, blunt force impacts, penetrating injuries, and surgery. Specific injuries covered include rib fractures, flail segments, pneumothorax, hemothorax, pulmonary contusions, lacerations, and fat embolism. Imaging techniques for evaluation such as CT, ultrasound, and aortography are also discussed.








































![Chest_xray_in_trauma and trauma[PS].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/chestxrayintraumaps-250501045112-cc7e42ce-thumbnail.jpg?width=640&height=640&fit=bounds)










































