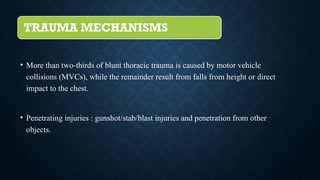
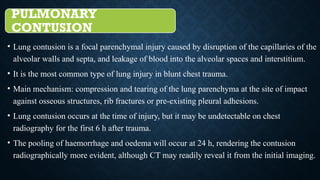
The document discusses the evaluation of thoracic and abdominal trauma using CT scans, highlighting the prevalence and types of injuries, such as pulmonary trauma from motor vehicle collisions and penetrating injuries. It details various imaging techniques, including chest radiography and contrast-enhanced CT, to assess injuries like pneumothorax, hemothorax, and lung contusions/lacerations. Additionally, it outlines the mechanisms of trauma, classifications of injuries, and diagnostic findings relevant to effective treatment and management of chest trauma.

![IMAGING TECHNIQUES FOR PULMONARY
TRAUMA
The chest radiograph is the primary initial screening examination performed in thoracic
trauma, although some centres also perform extended focused assessment in sonography
for trauma (eFAST).
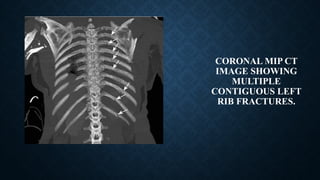
Chest radiography :1]Identify rib fractures
2] Foreign bodies/ballistic fragments
3] Contusions,
4] Pneumothorax
5] Hemothorax &mediastinal injuries
Contrast-enhanced CT :standard imaging tool in the evaluation of trauma patients.
(Greater sensitivity and specificity)](https://image.slidesharecdn.com/thoracicandabdominaltraumamodified-240811180241-5029115f/85/thoracic-and-abdominal-trauma-modified-pptx-5-320.jpg)




![• Flail chest: An injury that occurs typically
following a blunt trauma to the chest.
When three or more ribs in a row have
multiple fractures [atleast two] within each
rib, it can cause a part of your chest wall to
become separated and out of sync from the
rest of your chest wall.
• The diagnosis is clinical based on the
paradoxical motion during respiration,
which may result in ventilatory
compromise. More than 50% of cases
require surgical treatment and prolonged
mechanical ventilation.](https://image.slidesharecdn.com/thoracicandabdominaltraumamodified-240811180241-5029115f/85/thoracic-and-abdominal-trauma-modified-pptx-43-320.jpg)


























![Chest_xray_in_trauma and trauma[PS].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/chestxrayintraumaps-250501045112-cc7e42ce-thumbnail.jpg?width=640&height=640&fit=bounds)




































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)





![APPROACH TO FEVER IN PEDIATRICS[1].pptTT](https://cdn.slidesharecdn.com/ss_thumbnails/approachtofeverinpediatrics1-260125081456-d559e079-thumbnail.jpg?width=640&height=640&fit=bounds)


![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)


