Downloaded 116 times
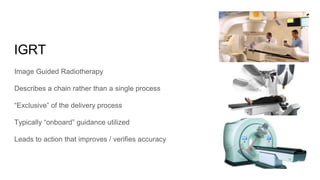
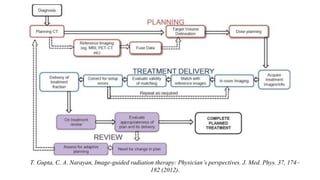
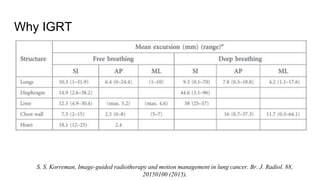

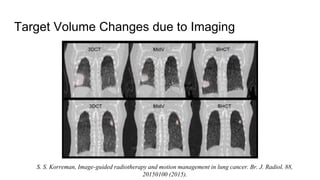
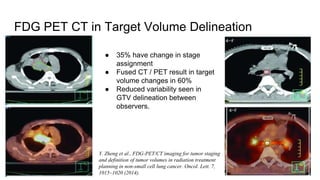
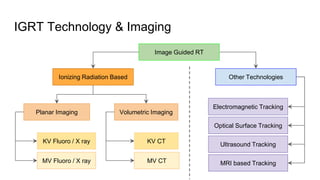
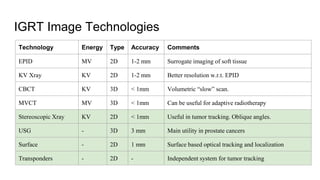



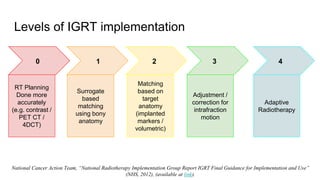
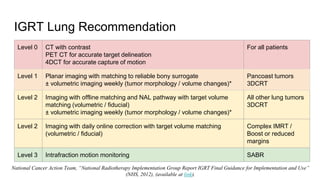
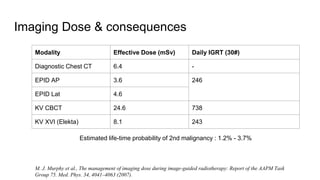

The document discusses the significance of Image-Guided Radiotherapy (IGRT) in lung cancer treatment, highlighting the challenges of tumor visibility and motion management. It outlines various imaging technologies, implementation levels, and emphasizes the need for specialized equipment and a collaborative approach for effective integration of IGRT in radiotherapy. Ultimately, IGRT contributes to improved accuracy and safety in targeting tumors while reducing doses to surrounding healthy tissues.



















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
