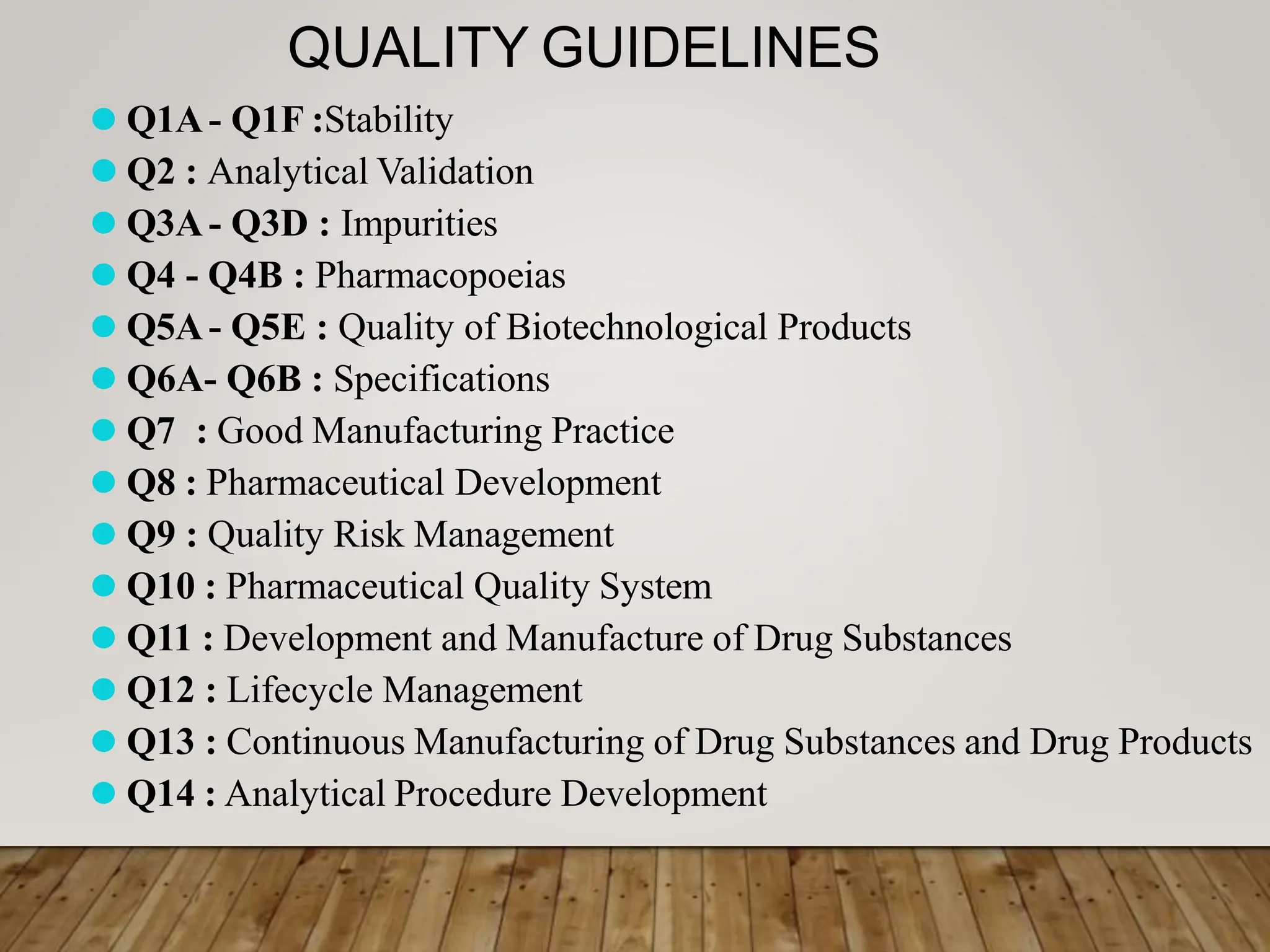
This document provides an overview of ICH guidelines. ICH is an international non-profit organization that brings together regulatory authorities and pharmaceutical industries from Europe, Japan, and the US to discuss technical requirements for drug development and registration. The document outlines the origins, objectives, members and processes of ICH. It also summarizes the various guidelines developed by ICH on quality, safety, efficacy, and multidisciplinary topics.