Downloaded 100 times

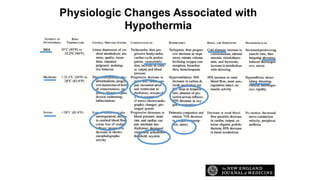

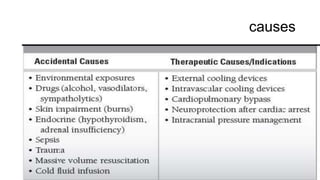



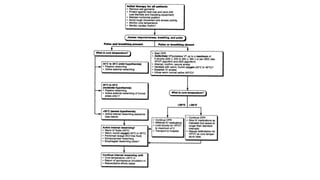


Hypothermia is common in trauma patients and those exposed to cold environments. It can be accidental, primary, secondary, or therapeutic. Mild hypothermia between 32-35 degrees Celsius is used for neuroprotection, while moderate (28-32 degrees) is used for cardiopulmonary bypass. Physiologic changes associated with hypothermia include coagulopathies, metabolic effects, hypokalemia, hyperglycemia, and effects on the cardiovascular, immune, and coagulation systems. Treatment follows the ABCDE approach - ensuring a patent airway, warming humidified oxygen, warm IV fluids, monitoring for hypoglycemia, and passive or active external rewarming depending on severity. Core rewarm


































































![Prehospital induced hypothermia post cardiac arrest jun 2010[1]](https://cdn.slidesharecdn.com/ss_thumbnails/prehospitalinducedhypothermiapost-cardiacarrestjun20101-120131131556-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)







































