This document discusses hypothermia and frostbite. Some key points:
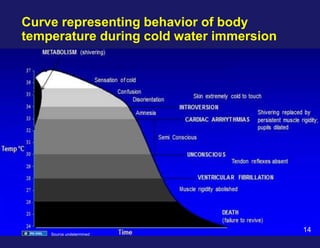
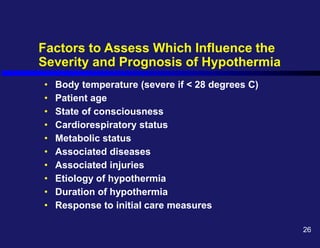
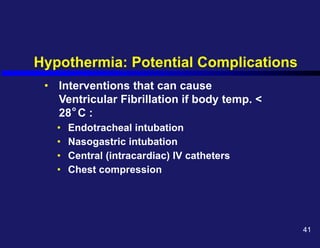
1. Hypothermia is defined as a body temperature below 35°C (95°F). Severe hypothermia is below 28°C. It can cause confusion, loss of consciousness, and death.
2. Risk factors for hypothermia include extremes of age, medical conditions, drugs/alcohol, malnutrition, and exposure to cold. The elderly are especially vulnerable due to thinner skin and reduced ability to shiver.
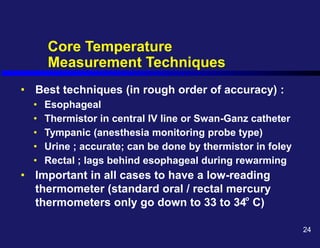
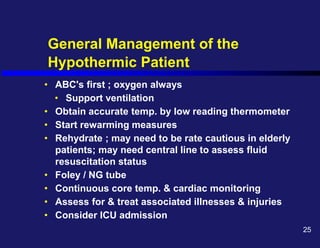
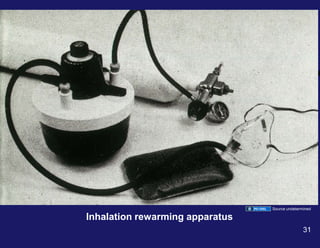
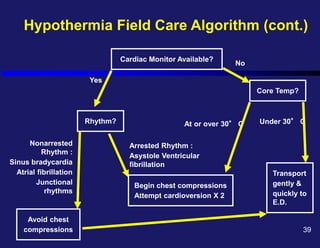
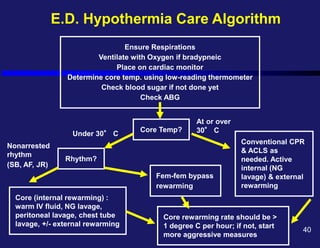
3. Rewarming techniques include warmed oxygen, IV fluids, gastric/rectal lavage, and external warming. The goal is to raise the core temperature over 1°C


































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
















![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

