Downloaded 57 times


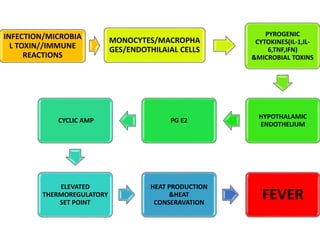
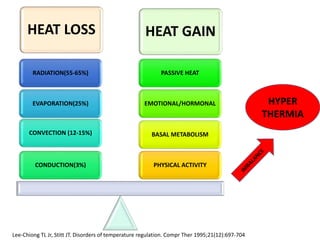
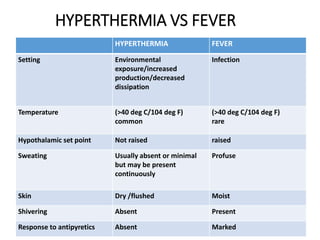
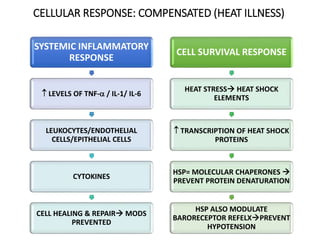
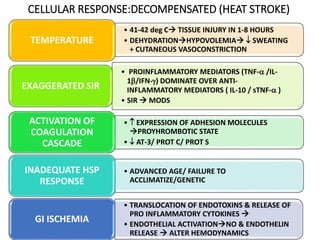
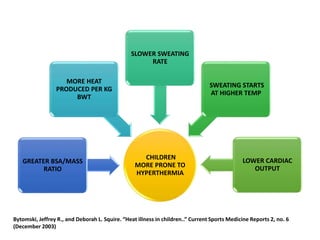
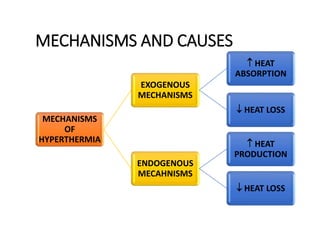


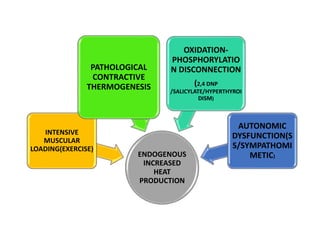
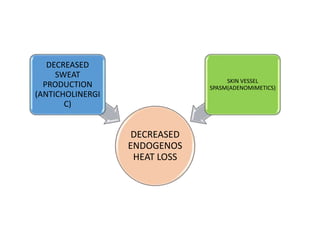

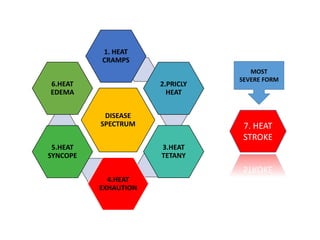


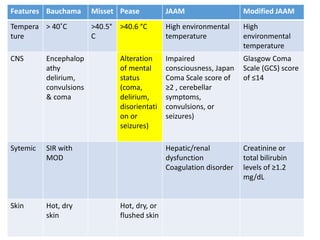










Hyperthermia and heat stroke are conditions caused by the body failing to regulate its core temperature. Hyperthermia occurs when the body gains too much heat or loses too little, while fever is a regulated increase in temperature by the hypothalamus in response to infection. Heat illnesses form a spectrum from mild heat cramps to the most severe, heat stroke, defined as a core temperature over 40°C with neurological dysfunction. Heat stroke results from a failure of thermoregulation during heat exposure that leads to systemic inflammatory response and multi-organ damage.














































































