Downloaded 84 times
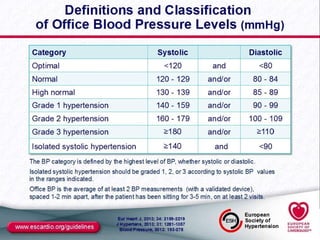
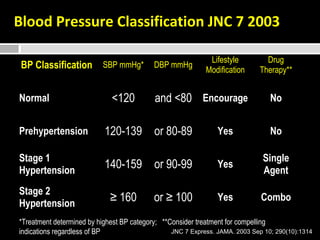
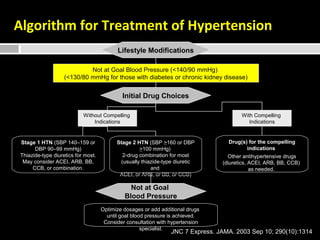
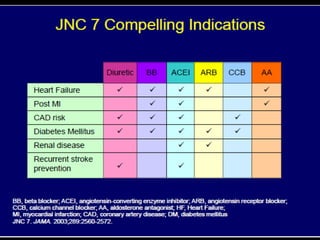
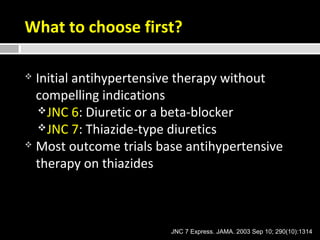
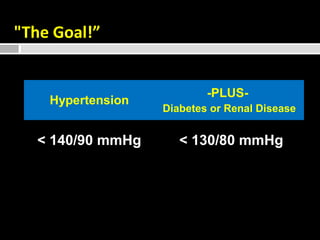

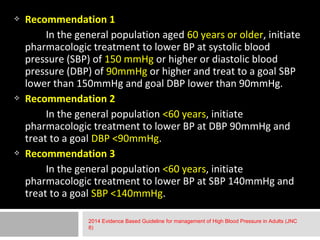
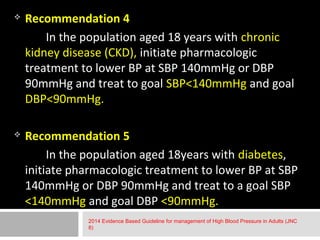
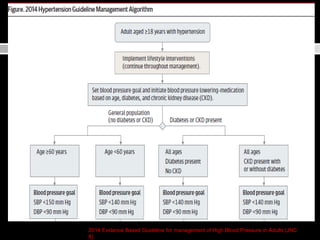
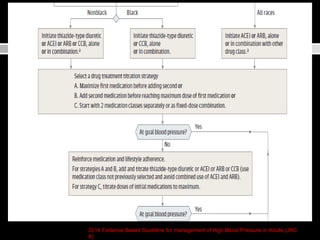
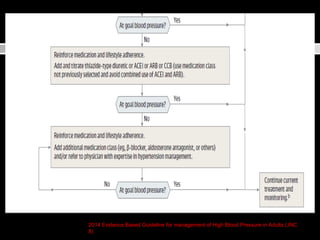
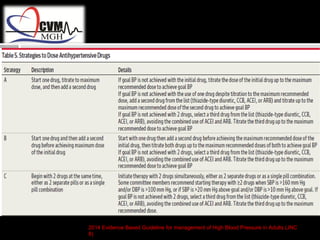
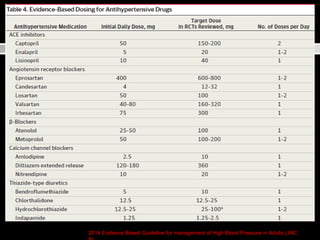
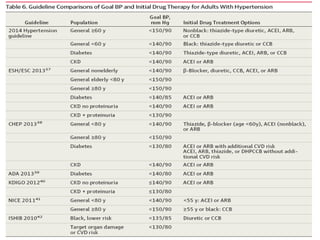
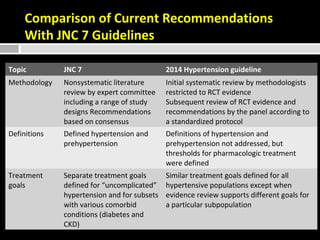
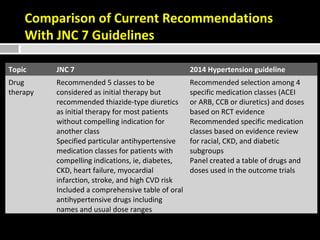
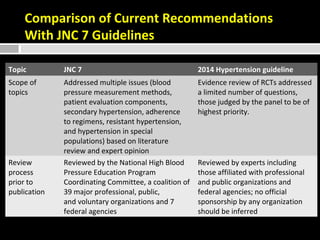

The document summarizes the key changes between the 2014 hypertension guidelines (JNC 8) and previous guidelines (JNC 7). The 2014 guidelines lower treatment thresholds based on rigorous evidence from randomized controlled trials. They recommend initiating treatment at SBP/DBP of 140/90 mmHg for those under 60, and 150/90 mmHg for those 60 and over. For those with diabetes or chronic kidney disease, the goal is SBP/DBP under 140/90 mmHg. Thiazide-type diuretics, ACE inhibitors, ARBs, calcium channel blockers are first-line treatments depending on population. The guidelines note limitations around scope and costs/adherence.





























































































