Downloaded 1,529 times



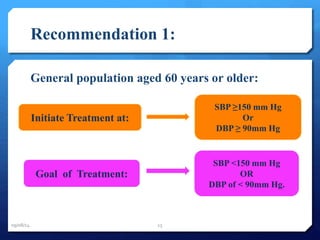



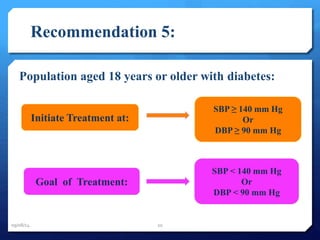

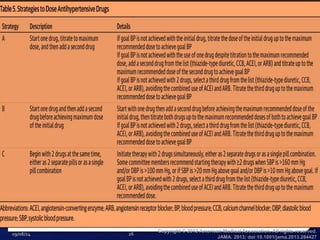

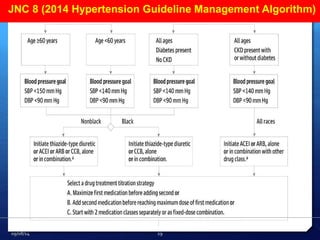
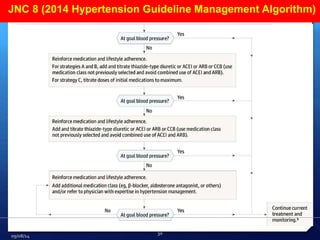

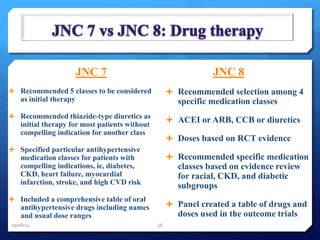
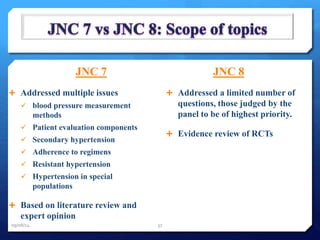

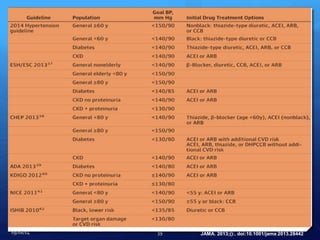


The document summarizes the key recommendations from JNC8, the Eighth Joint National Committee evidence-based guidelines for hypertension. Some of the main recommendations include: initiating treatment for those aged 60 or older with systolic blood pressure of 150 mm Hg or higher, or diastolic blood pressure of 90 mm Hg or higher; treating to a goal of under 150/90 mm Hg; and using thiazide diuretics, calcium channel blockers, ACE inhibitors, or ARBs as first-line treatment options. The guidelines are based on an extensive systematic review of randomized controlled trials on hypertension management.