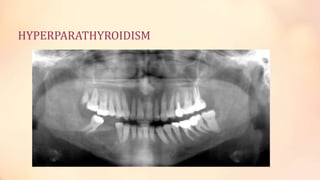
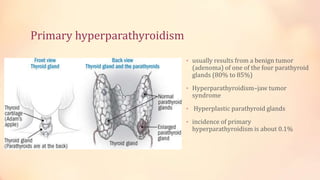
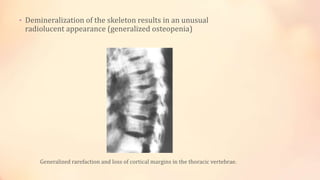
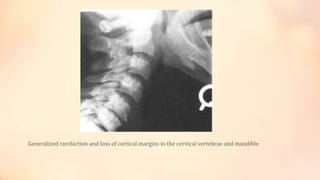
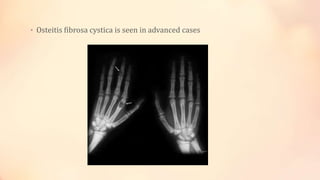
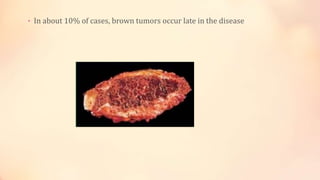
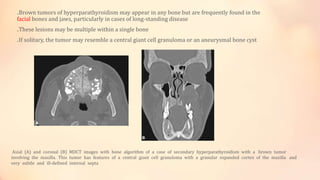
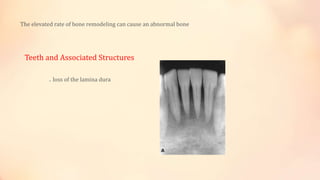
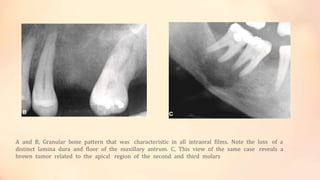
Hyperparathyroidism is a condition caused by excess parathyroid hormone that can lead to changes in bone structure and density. Primary hyperparathyroidism is usually caused by a benign tumor of the parathyroid glands and affects females more than males aged 30-60. Symptoms include those related to hypercalcemia like bone pain. Imaging may show features like brown tumors, osteopenia, and a "salt and pepper skull". Surgical removal of the tumor can resolve the condition and reverse changes except for sites of brown tumors.









































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)