
More Related Content
What's hot
What's hot (20)
Similar to HYPERTENSIVE RETINOPATHY - DR ARNAV SAROYA
Similar to HYPERTENSIVE RETINOPATHY - DR ARNAV SAROYA (20)
Recently uploaded
Recently uploaded (20)
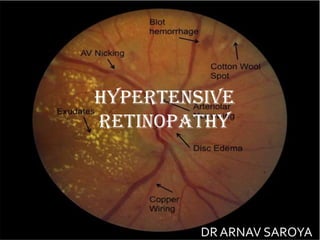
HYPERTENSIVE RETINOPATHY - DR ARNAV SAROYA
- 5. 1. Genetic factors can also play a role with certain genotypes associated with an increased risk of hypertensive retinopathy. 2. Smoking is considered to have a strong association with severe or malignant hypertensive retinopathy . 3. Renal dysfunction (persistent microalbuminuria and low creatinine clearance) in patients has shown to be a marker for hypertensive retinopathy and end-organ damage. 4. Arteriosclerotic changes of hypertensive retinopathy are caused by chronically elevated blood pressure, defined as systolic greater than 140 mmHg and diastolic greater than 90 mmHg. Hypertension is usually essential and not secondary to another disease process. ETIOLOGY
- 6. •Retinal blood vessels have distinct features, which differentiate them from other blood vessels • The absence of sympathetic nerve supply • Autoregulation of blood flow • Presence of blood-retinal barrier •Thus, an increase in blood pressure (BP) is transferred directly to the vessels which initially constrict. • However, a further increase in BP overcomes this compensatory tone and damage to the muscle layer and endothelium ensues.
- 18. Bonnet’s sign: Banking of the retinal vein distal to the AV crossing
- 19. Decrease in the arteriovenous ratio to 1:3 ( the normal ratio is 2:3).
- 34. Collaterals.
- 44. •Siegrist's streak: RPE hyperplasia over choroidal infarcts
- 65. COMPLICATIONS • Retinal artery occlusion • Retinal vein occlusion • Macro aneurysm of retinal arteriole • Diabetic retinopathy (DR): Both hypertensive retinopathy and DR together in a patient is called as mixed retinopathy. HTN is also known to be a major risk factor for the progression of DR. • Anterior ischemic optic neuropathy • Age-related macular degeneration • Glaucoma • Retinal arteriolar emboli • Epiretinal membrane formation • Cystoid macular edema
- 66. MANAGEMENT • Systemic hypertension should be controlled as a primary measure for Hypertensive retinopathy. • Change in lifestyle with reduction of general risk factors (salt restriction, avoidance of tobacco) help in controlling hypertension. • Drugs may be used from groups like: • – Diuretics. • – Beta blockers. • – Angiotensin converting enzyme inhibitors. • – Calcium channel blockers. • – Angiotensin receptor antagonists.
- 67. •Patients with severe hypertensive retinopathy are at increased risk of coronary artery disease, stroke or peripheral vascular disease. Arteriosclerotic changes increases the risk of retinal macroaneurysms, retinal artery or vein occlusion. Visual acuity may be reduced due to involvement of optic nerve and macula. •Hypertensive retinopathy with vision threatening complication: Vision threatening complications like retinal oedema may be treated with laser therapy or intravitreal injection of vascular endothelial growth factor (VEGF) drugs.
Editor's Notes
- caused by chronically elevated blood pressure, defined as systolic greater than 140 mmHg and diastolic greater than 90 mmHg
- Severity and duration of htn are directly related to incidence of htn retinopathy .
- In a study by kabedi et al – htn retino in 83.6 % out of total hypertensive patients and chronic kidney disease – most significant factor to predict severe htn ret. Malignant htn – above 180/120
- SECONDARY HTN – bycondtns affecting the kidneys , arteries , heart or endocrine system. Secondary hypertension may be caused by an underlying disease such as: – Primary hyperaldosteronism. – Cushing’s syndrome. – Phaeochromocytoma. – Renal vascular or renal parenchymal disease. – Coarctation of aorta. – Hyperthyroidism. – Hyperparathyroidism
- acute effects of systemic arterial hypertension are a result of vasospasm to autoregulate perfusion[2]. The chronic effects of hypertension are caused by arteriosclerosis and predispose patients to visual loss from vascular occlusions or macroaneurysms