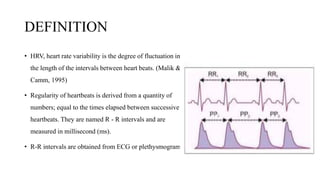
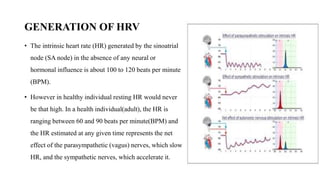
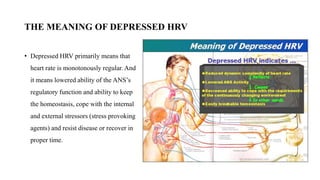
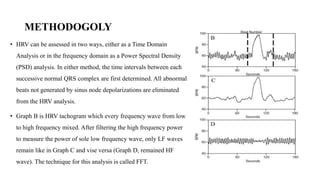
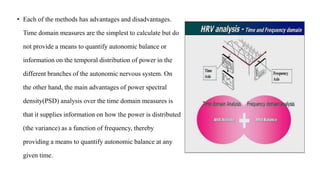
This document discusses heart rate variability (HRV), including definitions, how it is generated, methodology and terminology used in HRV analysis. HRV is the variation in time between each heartbeat and can provide information about the autonomic nervous system. HRV is analyzed using time domain and frequency domain methods to measure parameters like SDNN, LF, HF, and LF/HF ratio which indicate sympathetic and parasympathetic activity. Depressed HRV indicates reduced autonomic regulation and ability to cope with stress. HRV analysis can be used clinically to assess fitness, treatment effectiveness, and stress levels.