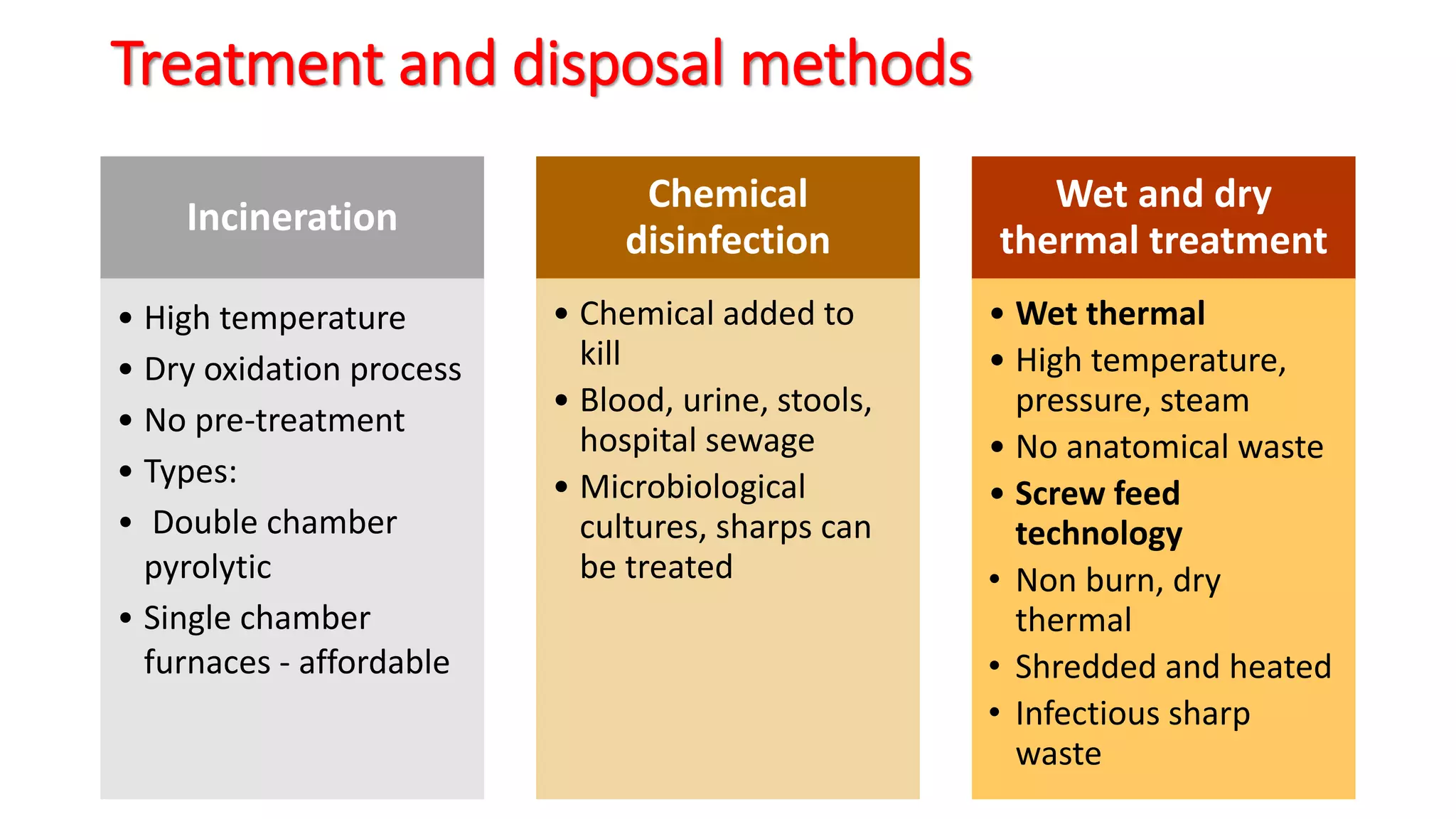
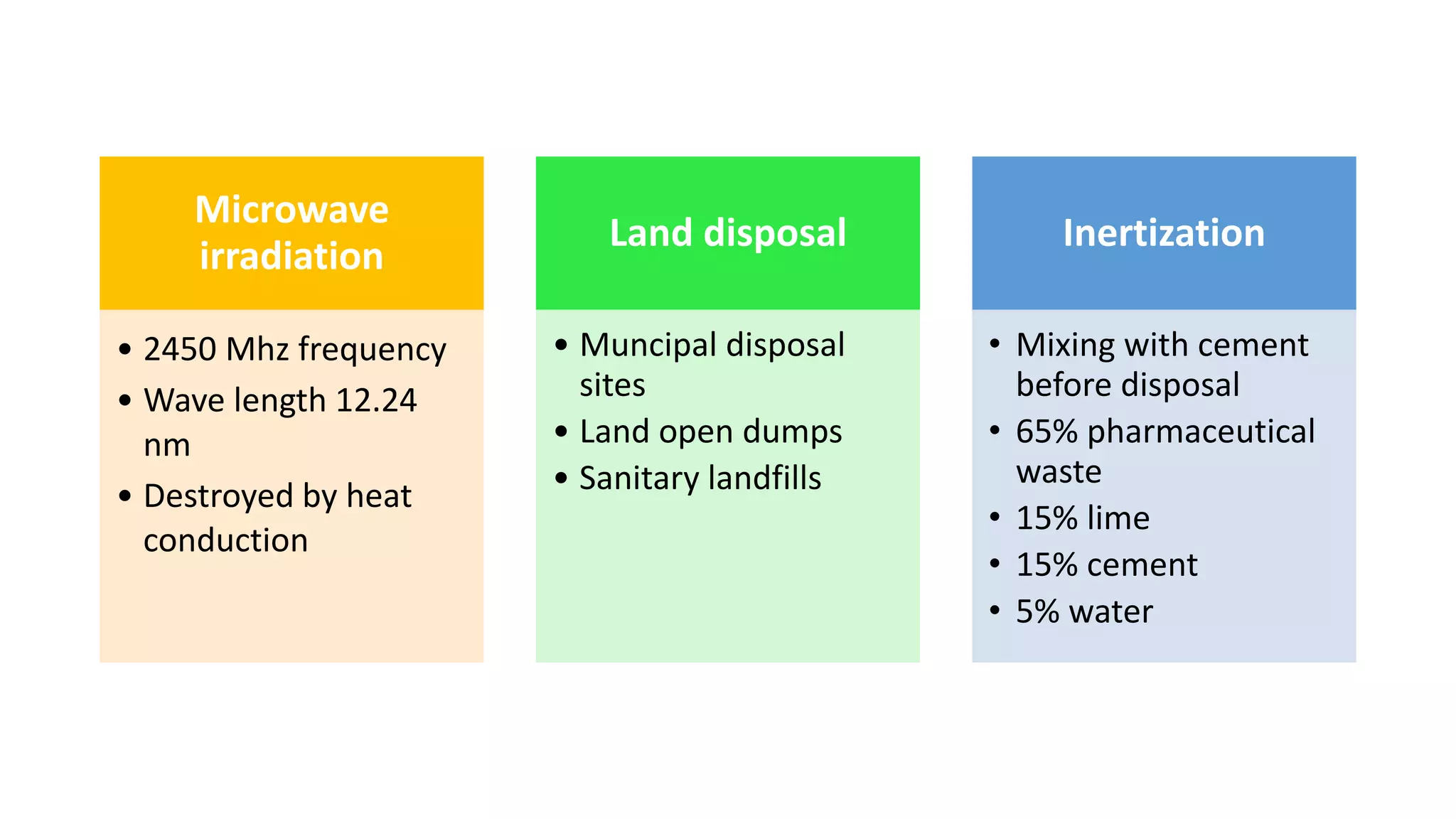
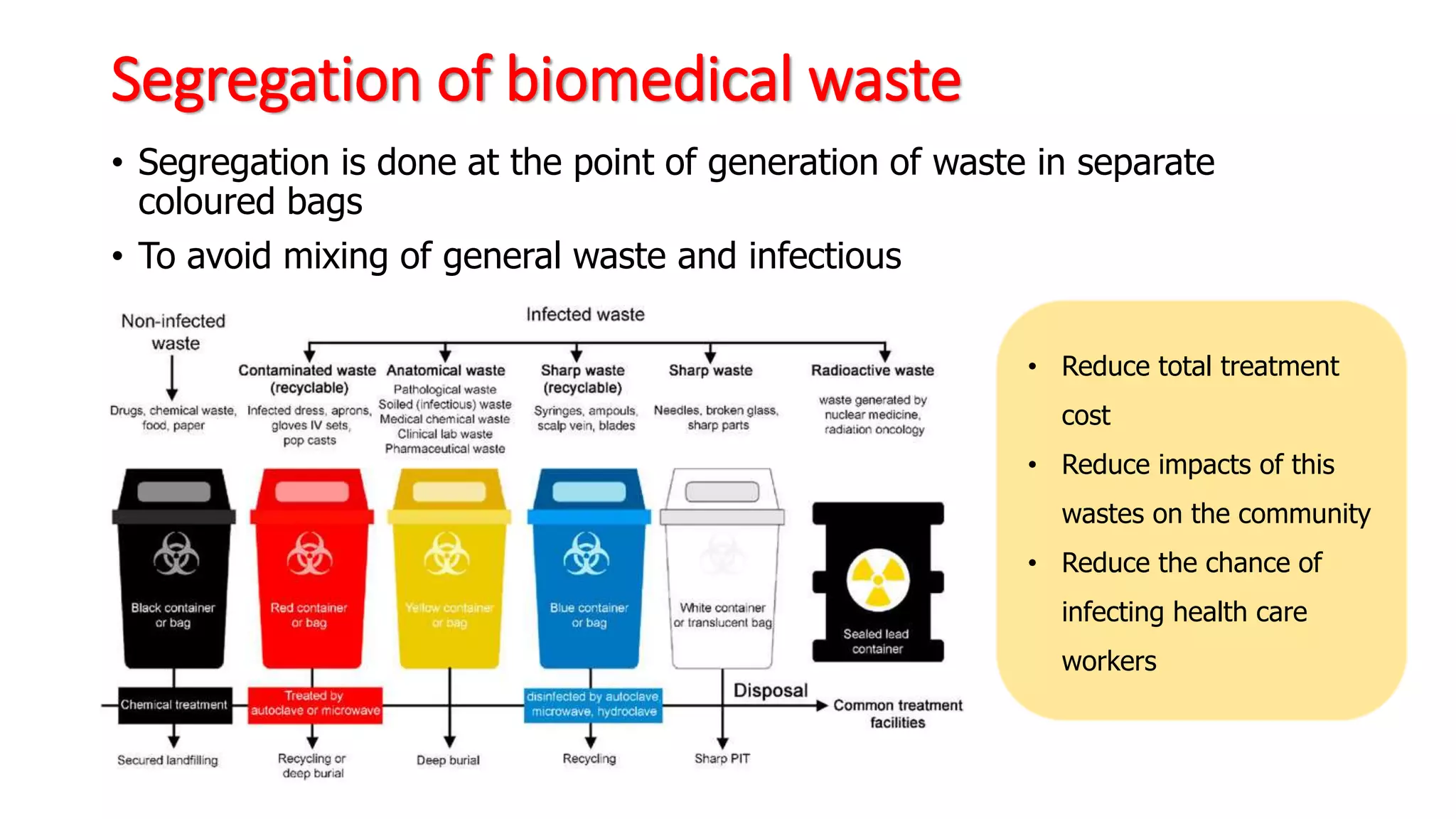
This document summarizes healthcare waste management. It defines biomedical waste and notes that most waste (75-90%) is non-hazardous while 10-25% is hazardous. Sources of healthcare waste include hospitals, clinics, laboratories, and more. Treatment and disposal methods discussed include incineration, chemical disinfection, wet/dry thermal treatment, microwave irradiation, and land disposal. The advantages and disadvantages of different treatment methods are also outlined. The document describes how waste should be segregated by category and color-coded bags or containers for treatment and disposal.


![Definition
• Biomedical waste (BMW)– Any waste generated during the
odiagnosis, treatment or immunization of human beings or animals,
oor in research activities pertaining thereto
oor in the production or testing of biologicals
[BMW Management and Handling rules, 1998 of India]
• 75 – 90% non-risk or general health care waste
• 10 – 25% hazardous waste](https://image.slidesharecdn.com/hospitalwastemanagement-230601101527-7806acf0/75/HOSPITAL-WASTE-MANAGEMENT-pptx-3-2048.jpg)