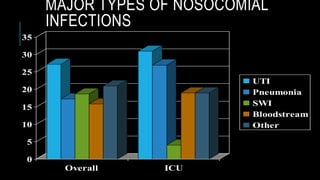
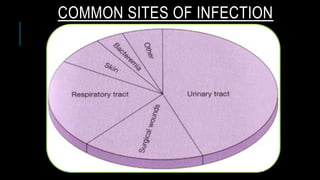
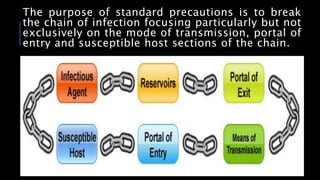
This document summarizes nosocomial infections and their control. It defines nosocomial infections as those acquired in a hospital by a patient admitted for another reason. The most common types are urinary tract infections, surgical site infections, and pneumonia. Transmission occurs via contact, droplets, and contaminated equipment. Proper hand hygiene, isolation, sterilization of equipment, and environmental cleaning are effective prevention strategies.