The document discusses HIV/AIDS, including:
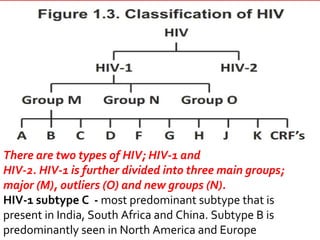
- HIV was identified as the cause of AIDS in 1983.
- HIV is transmitted through unprotected sex, contaminated blood, and from mother to child.
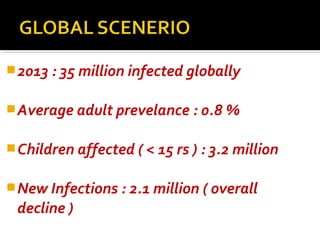
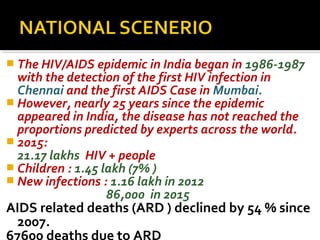
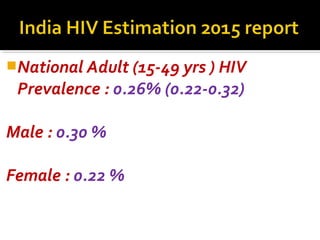
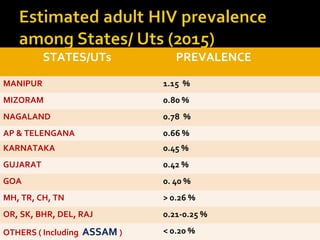
- India's HIV epidemic began in the 1980s, with over 2 million new infections globally in 2013.
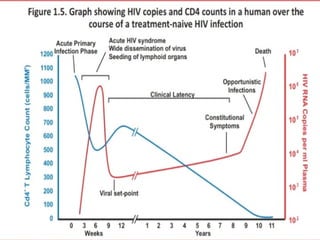
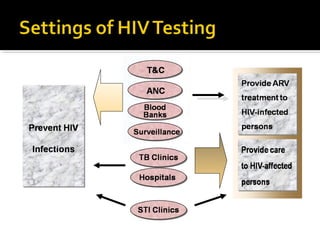
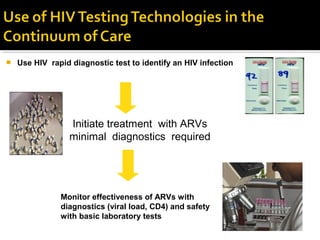
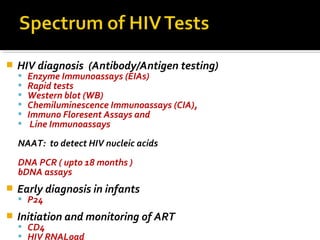
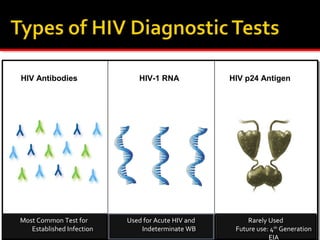
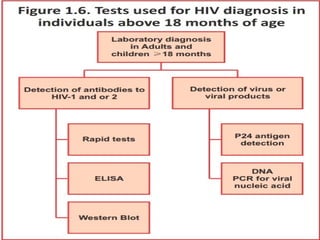
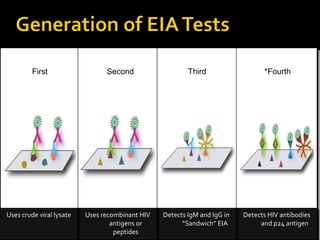
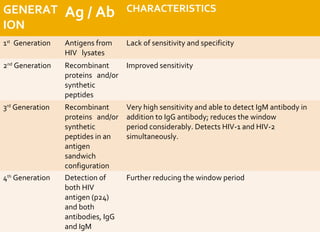
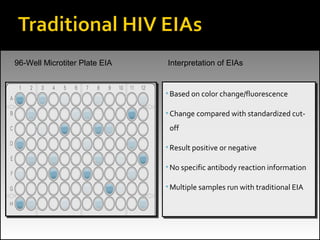
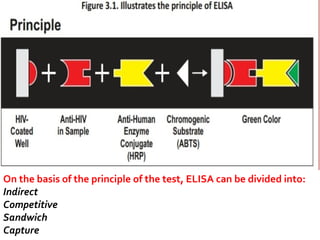
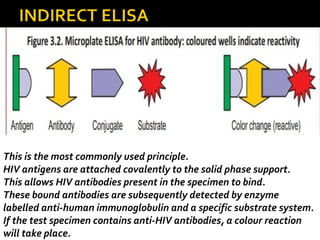
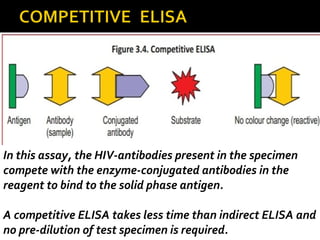
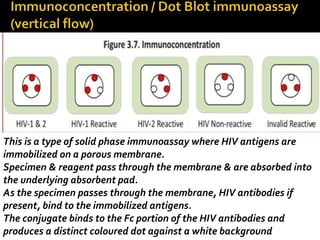
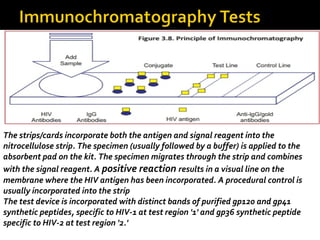
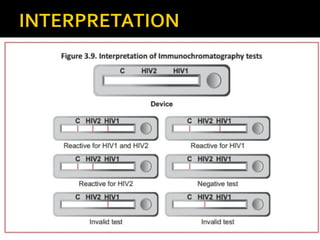
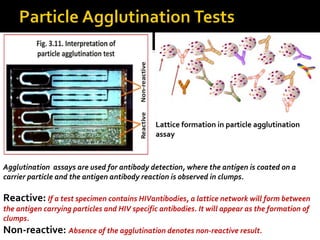
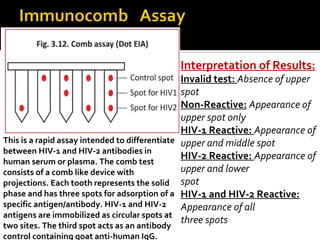
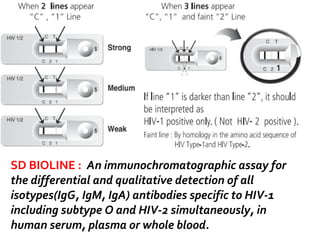
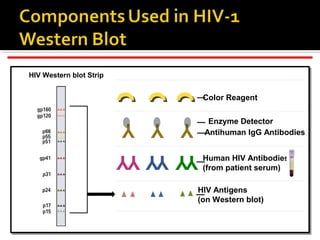
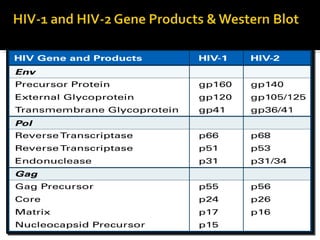
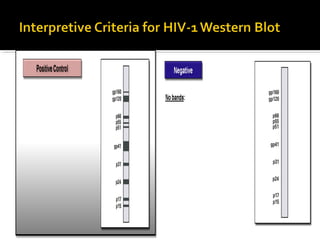
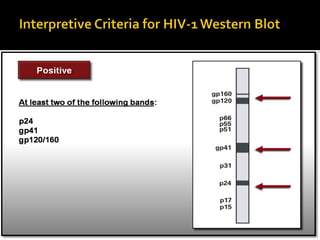
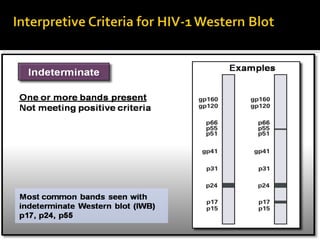
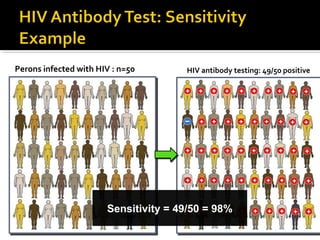
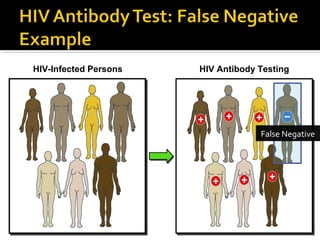
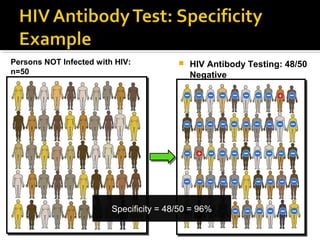
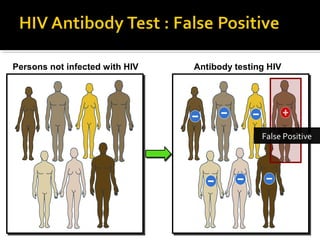
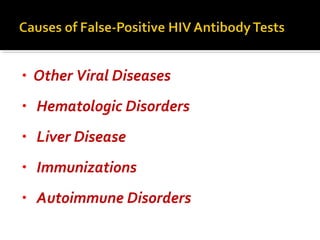
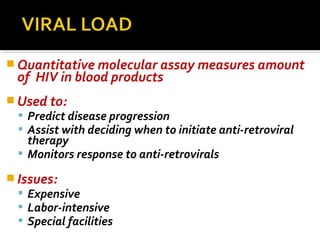
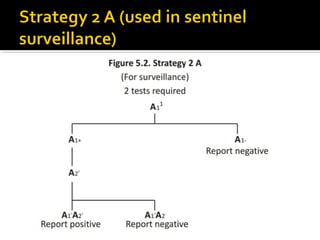
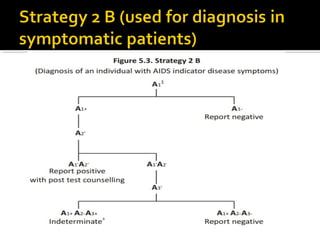
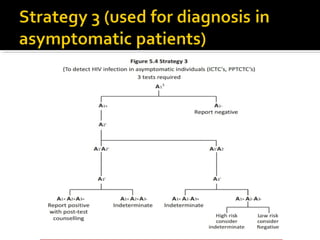
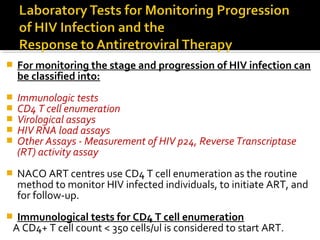
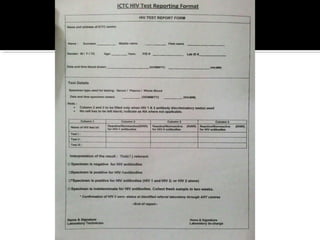
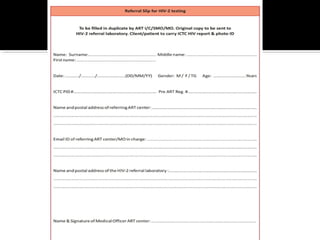
- HIV diagnosis involves antibody and antigen tests, while treatment and monitoring involves CD4 counts and viral load tests.