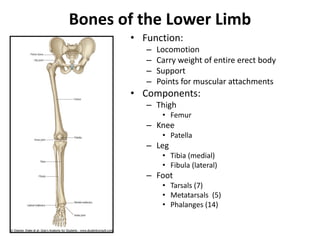
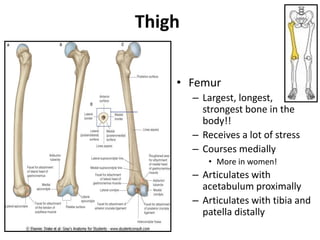
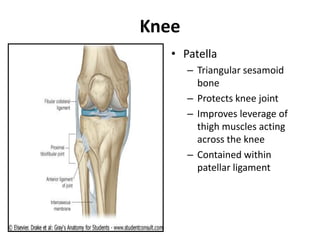
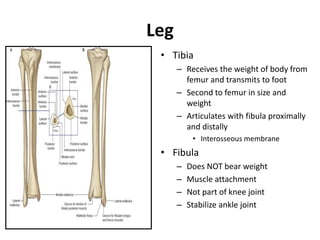
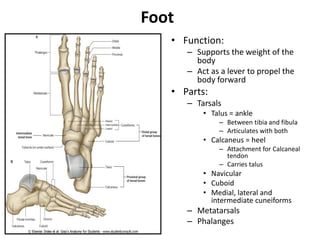
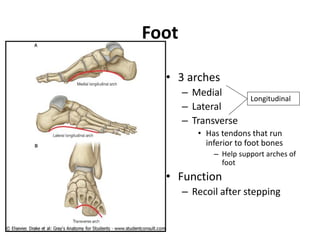
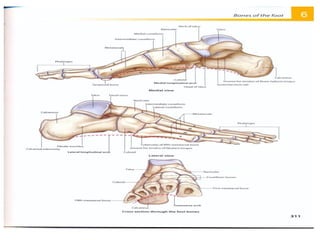
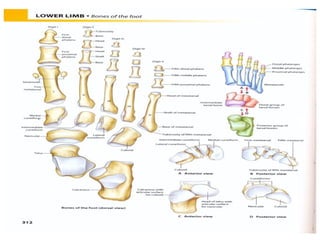
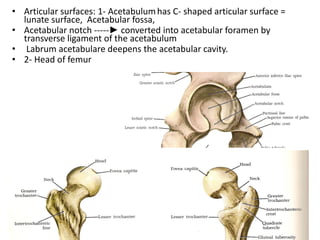
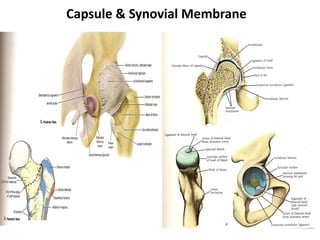
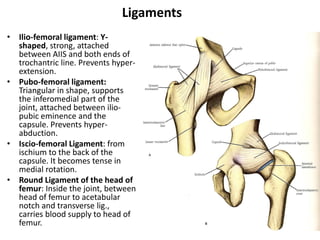
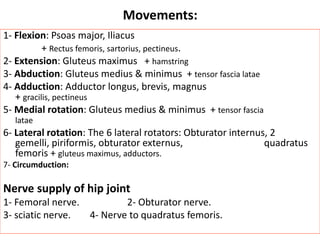
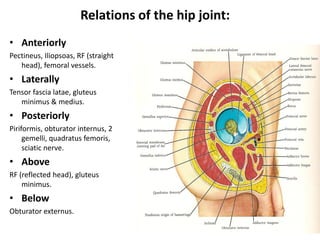
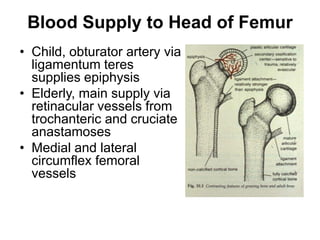
This document provides an overview of the lower limb skeleton and hip joint, detailing the anatomical structures, their functions, and their movements. It discusses the bones in the thigh, knee, leg, and foot, as well as the hip joint's stability, blood supply, and related musculature. Key points include the significant roles of ligaments, muscles, and the implications of injuries or pathologies affecting the hip region.