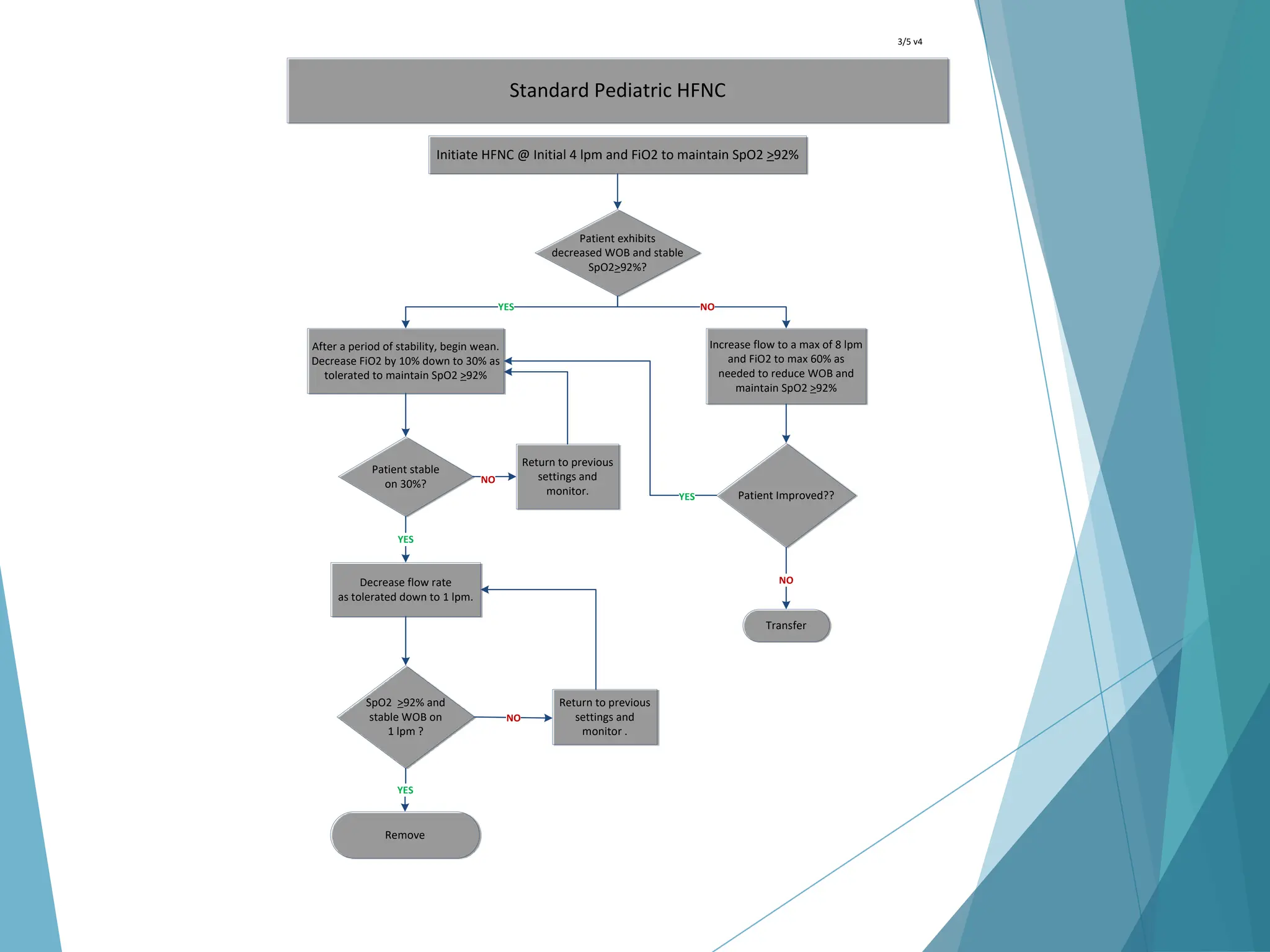
The webinar focuses on managing high flow nasal cannula (HFNC) therapy for bronchiolitis patients outside ICU settings. Key objectives include understanding the physiologic mechanisms of HFNC, identifying suitable patients, and discussing weaning protocols to enhance patient care. The presentation also emphasizes adapting management pathways to improve outcomes and reduce hospitalization duration.