Downloaded 18 times
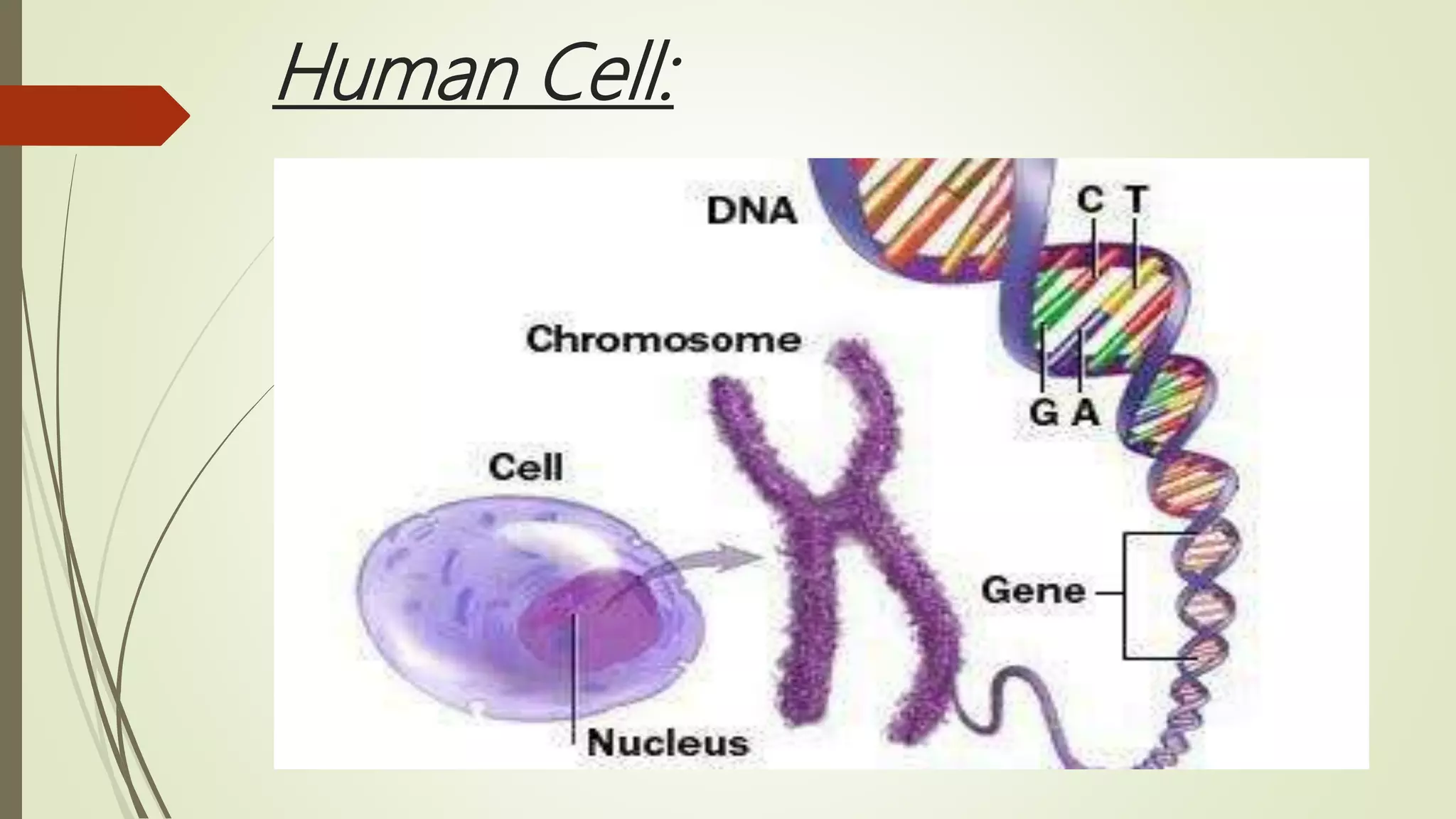
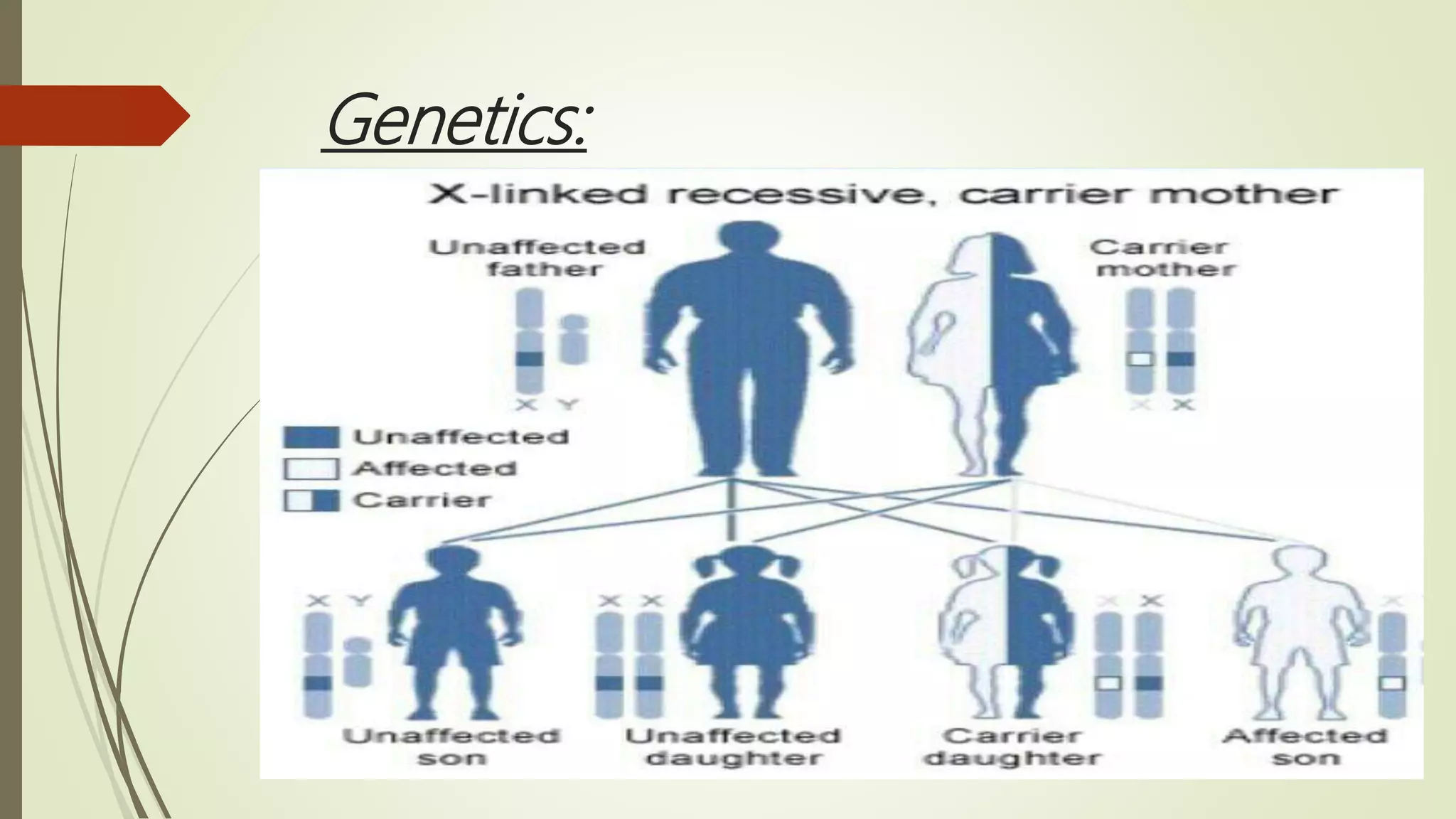
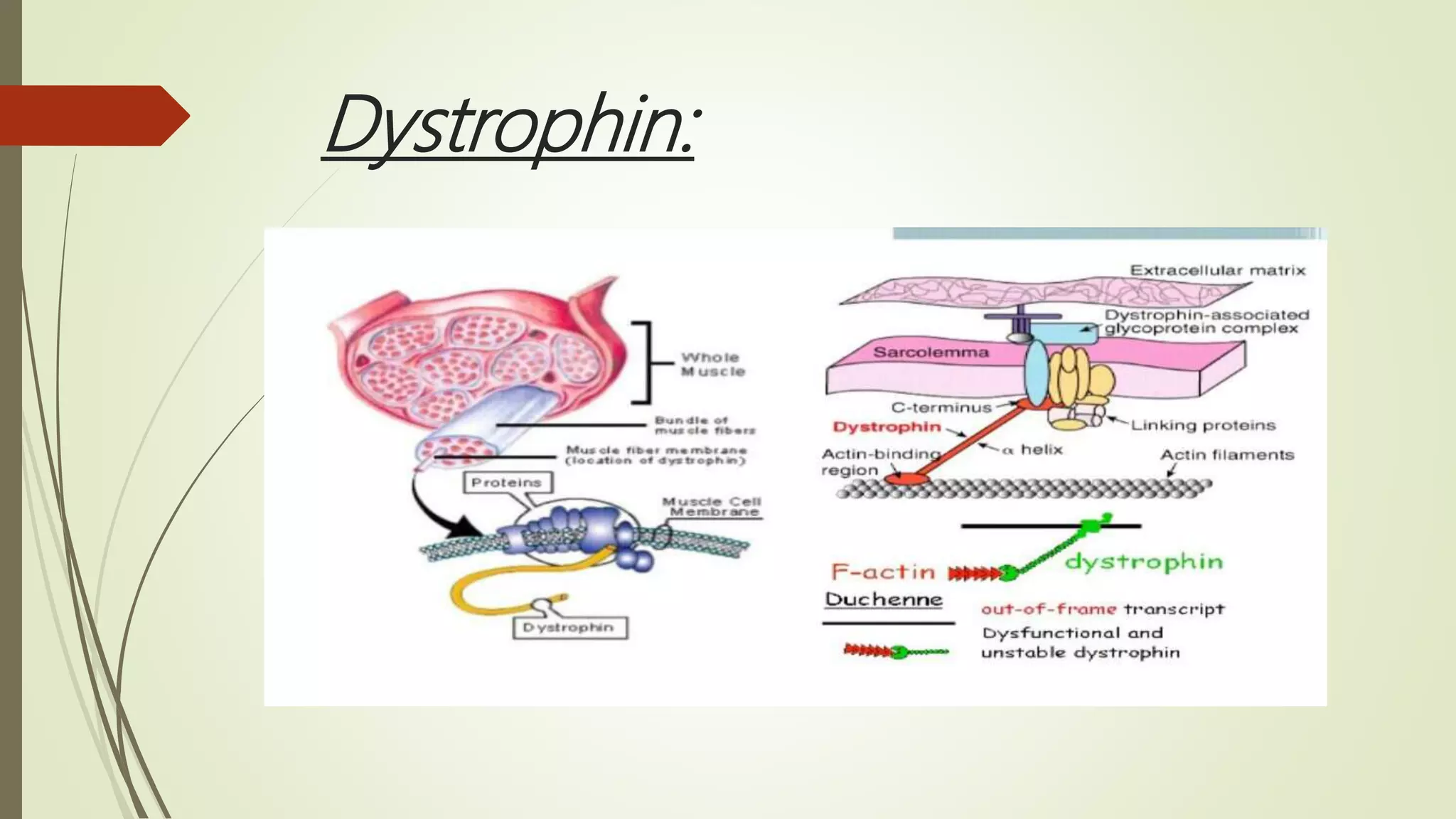
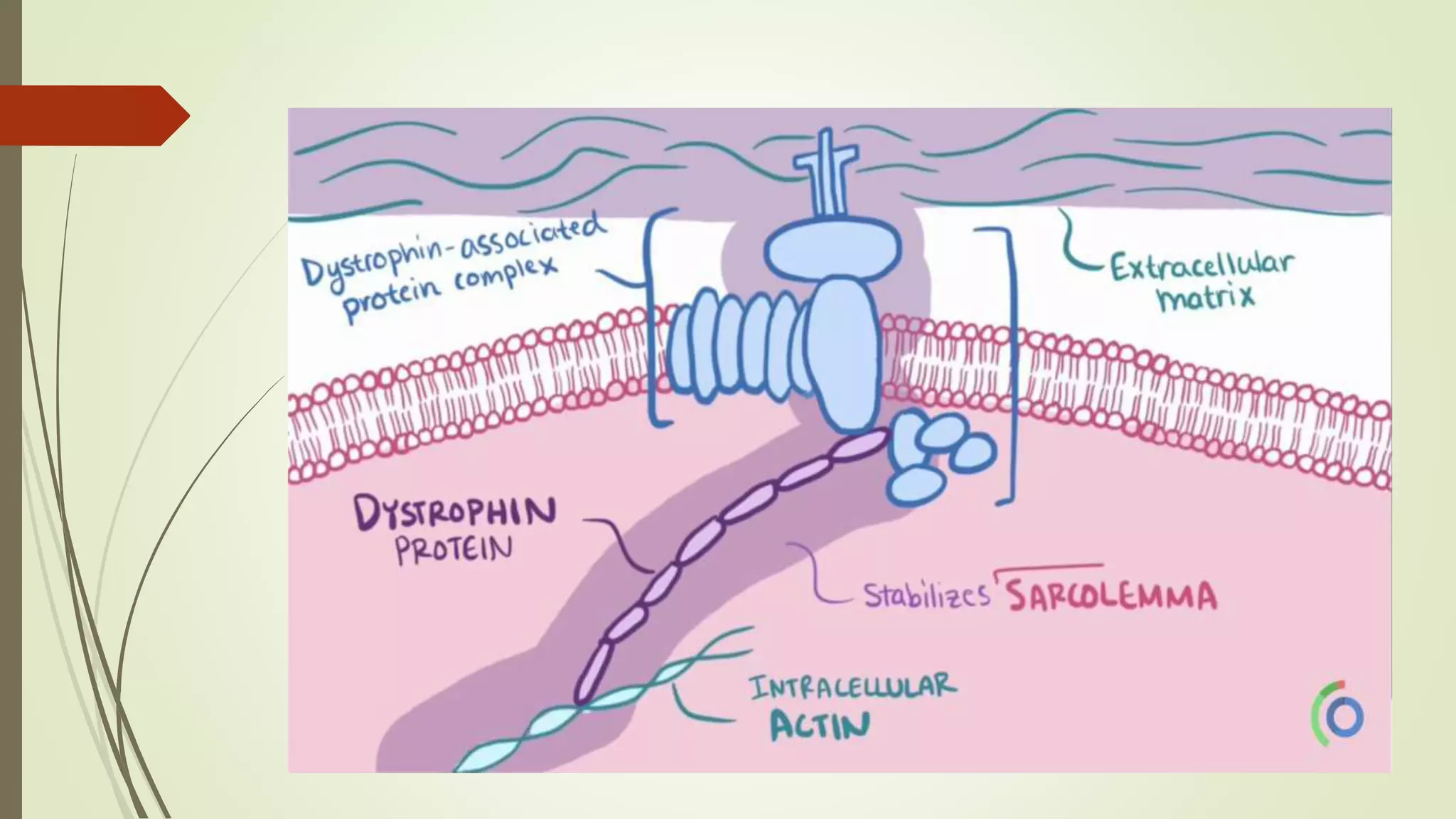
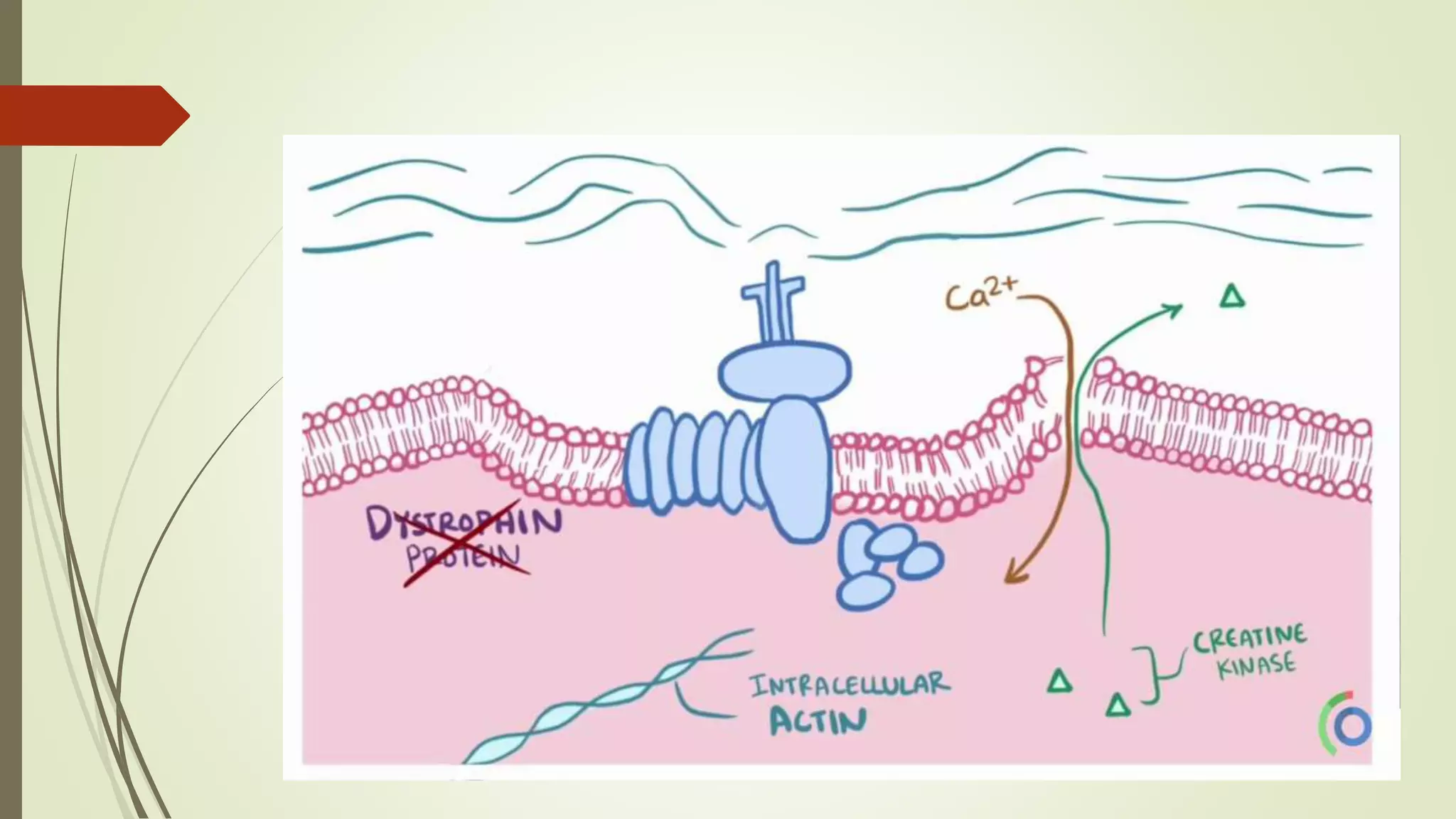
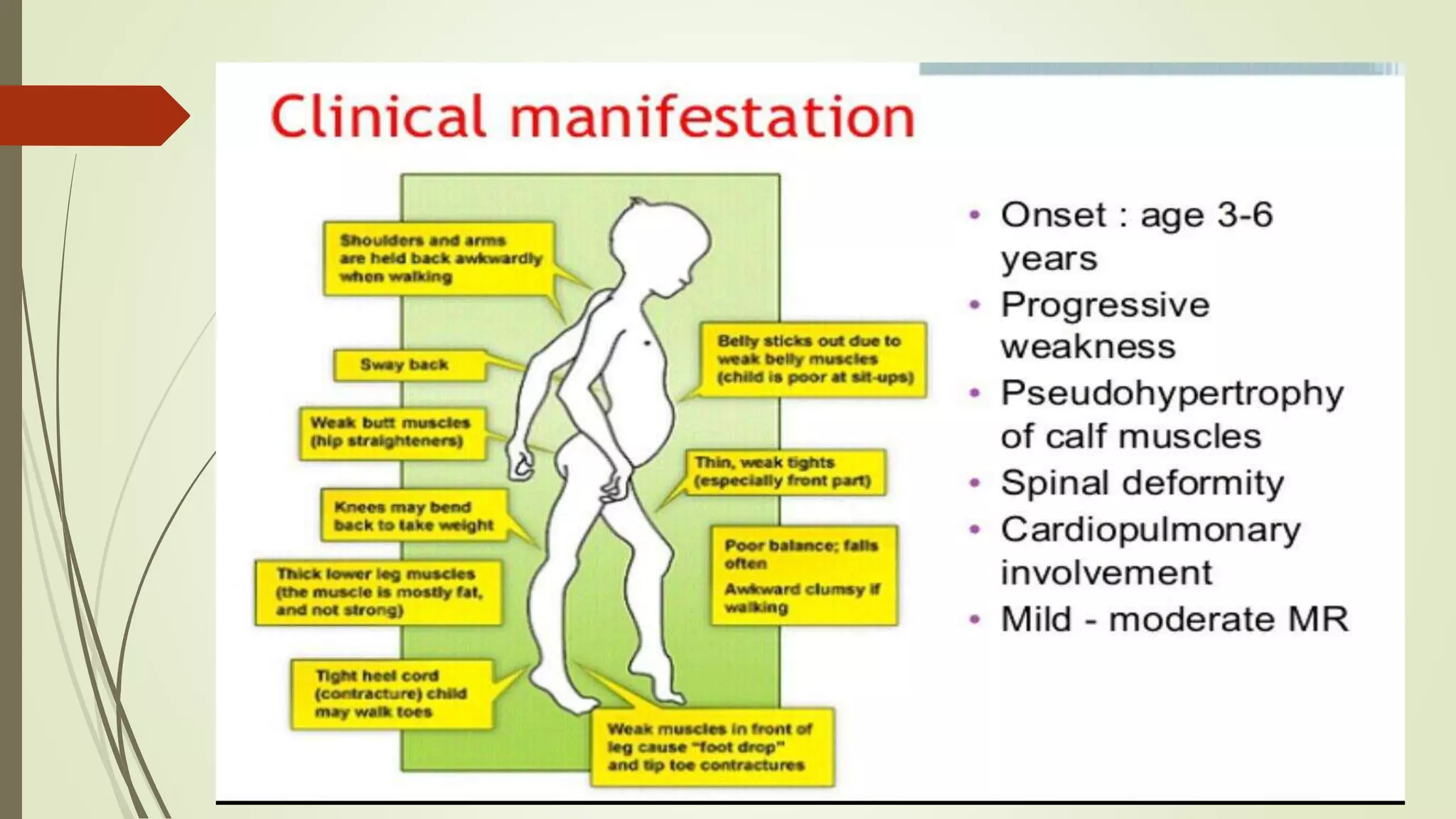


Muscular dystrophy is a group of inherited muscle diseases characterized by progressive weakening and breakdown of skeletal muscles. It results from genetic defects in proteins like dystrophin that help keep muscle cells intact. The dystrophin gene is located on the X chromosome, so the disease is often X-linked and affects males more severely. Over time, muscle cell damage leads to increasing difficulty with movements like walking, and can impact breathing or heart function in later stages. While there is no cure, treatment focuses on physical therapy, bracing, and other approaches to manage symptoms and improve quality of life.











































































