Downloaded 12 times



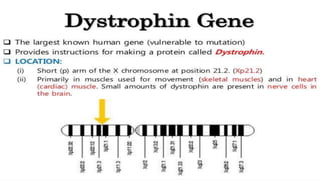
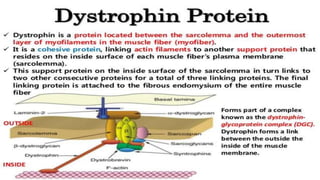
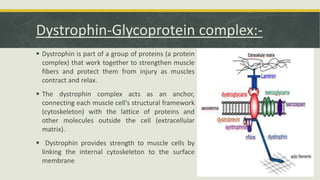
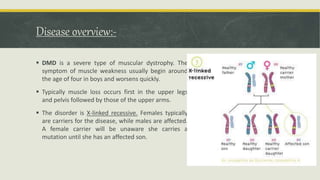



This document discusses Duchenne muscular dystrophy (DMD), a genetic disorder characterized by progressive muscle degeneration and weakness. It is caused by mutations in the dystrophin gene that result in little to no dystrophin protein. Without dystrophin, muscle fibers are damaged and die, leading to muscle weakness, loss of ambulation, and often premature death. The document covers the role of dystrophin in muscle cells, genetic causes, signs and symptoms, diagnostic testing, current treatments focused on symptom management, and associated health complications.



































































