Downloaded 18 times


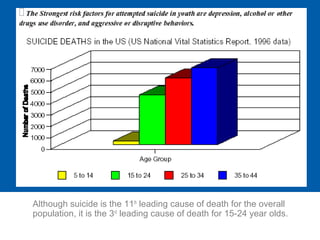



This document discusses adolescent depression, including its history, scope, causes, clinical manifestations, suicide risk, and management. It notes that depression is a common and serious medical illness in adolescents, with a prevalence of 4-8% having experienced depression in the past year. Left untreated, adolescent depression can lead to suicide, which is a leading cause of death among youth. The document explores the complexities in diagnosing and treating depression in adolescents due to developmental factors and outlines approaches to assessing and managing adolescent depression.





















![Somatic Symptom and Related Disorders [2020]](https://cdn.slidesharecdn.com/ss_thumbnails/ssrdv1-200526002841-thumbnail.jpg?width=640&height=640&fit=bounds)
































































