What is Impulsivity?
Rapid, unplanned reactions to stimuli before complete
processing of information.
Decreased sensitivity to negative consequences of behavior.
Lack of regard for long-term consequences.
Impulsivity often has an impact, not only on the impulsive
individual, but also on others.
[F. Gerard Moeller, Ernest S. Barratt,2001]
Failure to inhibit behaviors motivated by reward.
[Grant et al.2006]
What is Compulsivity?
Failure to suppress repetitive behaviors designed to relieve
tension or reduce a negative emotion state.
[Grant et al.2006]
Desire to avoid harm.
[Fineberg et al., 2010]
7.
What is Spectrumdisorder?
“Not a unitary disorder but rather syndrome composed of
subgroups”
Includes a range of linked conditions
The different elements of a spectrum either have a similar
appearance or are thought to be caused by the same
underlying mechanism.
Bipolar spectrum
Schizophrenia spectrum
Obsessive compulsive spectrum
8.
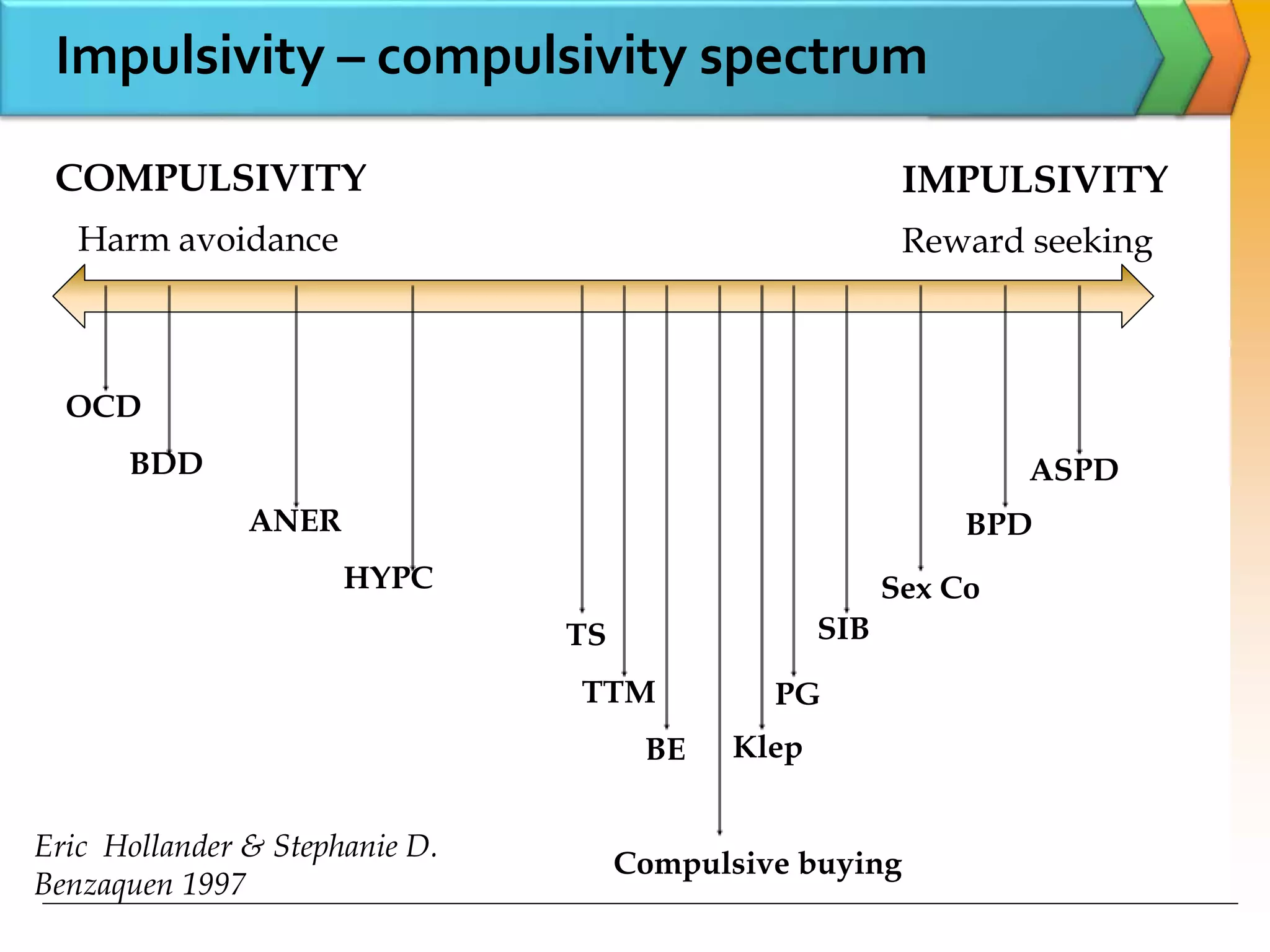
Impulsivity – compulsivityspectrum
IMPULSIVITY
Harm avoidance Reward seeking
COMPULSIVITY
OCD
BDD
ANER
HYPC
TS
TTM
BE
Compulsive buying
Klep
PG
SIB
Sex Co
BPD
ASPD
Eric Hollander & Stephanie D.
Benzaquen 1997
MCQs
Which ofthe following is not listed in ‘Habit and
Impulse control disorder’ in ICD 10?
A. Pathological Stealing (Kleptomania)
B. Pathological Gambling
C. Pathological fire setting (Pyromania)
D. Trichotillomania
E. Problematic internet use
Answer: Problematic Internet Use
11.
Which disorderhas been added to category
Impulse Control Disorder in ICD 11?
A. Problematic Internet Use
B. Compulsive sexual behavioural disorder
C. Exercise Addiction
D. Gaming Disorder
E. Food addiction
Answer: Compulsive sexual behavioural
disorder
MCQs
12.
Impulse control disorder…ICD-10
F60-F69:Disorders of adult personality and behavior
F63: Habit and Impulse Disorder
Repeated acts that have no clear rational motivation.
Generally harm patients own interest & those of other people.
Behavior is associated with impulses to action that can not be
controlled.
The WorkingGroup has recommended that a grouping
of impulse control disorders be retained in ICD-11.
Impulse control disorders would therefore include
1. Pathological gambling
2. Intermittent explosive disorder
3. Kleptomania
4. Pyromania
5. Compulsive sexual behaviour disorder. (In ICD- 10 it
was ‘Excessive Sexual Drive’)
ICD 11
16.
Trichotillomania- WorkingGroup has recommended it to
be moved to the grouping of obsessive-compulsive and
related disorders in ICD-11
Skin picking (excoriation) disorder also be added with
Trichotillomania.
ICD 11
Which ofthe following neurological condition is
associated with increased rate of Impulse
Control Disorder?
A. Motor Neuron Disease
B. Alzheimer's Dementia
C. Seizure Disorder
D. Parkinson’s Disease
E. Head Injury
Answer: Parkinson’s Disease
MCQs
19.
Prevalence in generalpopulation
791 students were screened for ICD.
Prevalence of one lifetime ICD was 10.4%,two was 1.5%.
[Brian L. Odlaug 2010]
Disorder Prevalence in
percentage
Trichotillomania 3.92
Compulsive sexual behavior 3.67
Compulsive buying 1 .90
Pyromania 1.01
Pathological gambling 0.63
Intermittent explosive disorder 0.51
Kleptomania 0.38
20.
Rates of OCDin ICDs
Gambling 1% to 20%
Kleptomania 7% to 60%
Pyromania 4.5%
Compulsive sex 14%
Excessive Internet use 15% to 20%
Compulsive buying 35%
21.
ICD among Parkinson'sdisease
Around 3000 PD patients interviewed for ICD
More common in patients treated with a dopamine agonist
than in patients not taking a dopamine agonist [odds ratio:2.72]
[Daniel Weintraub 2010]
Prevalence in %
Any ICD 13.6
Pathological Gambling 5
Compulsive sexual behavior 3.5
Compulsive buying 5.7
Binge eating 4.3
Neurotransmitter associatedwith impulsivity?
A. Serotonin
B. Dopamine
C. GABA
D. Glutamate
E. All of the above
Answer: All of the above
MCQs
24.
Incentive sensitizationtheory-repeated drug exposure leads
to a sensitization (reverse tolerance) of the incentive-
motivational properties of behavior and behavior-related
cues, where NAcc & Dopamine role has been implicated
Opponent process theory-the first involves affective or
hedonic habituation, the second process is an affective or
hedonic withdrawal
Neuroplasticity theory- contributing to addiction is the
recruitment of habit-based neurocircuitry throughout
repeated drug exposure
[Christopher M. Olsen 2011]
Theories of behavioral plasticity & addiction
25.
A-B-C model forICD
Affective
dysregulation
Behavioral
addiction
Cognitive
dyscontrol
A
B
C
Dan J. Stein et al. 2006
Which ofthe following psychiatric condition is
more closely associated with Pathological
Gambling?
A. Major Depression
B. Schizophrenia
C. Alcohol dependence syndrome
D. Adult ADHD
E. None of the above
Answer: Alcohol Dependence Syndrome
MCQs
31.
Pathological Gamblingis more commonly seen
in type of personality disorder?
A. Antisocial
B. Dependent
C. Borderline
D. Schizoid
E. Obsessive Compulsive
Answer: Antisocial
MCQs
32.
Which ofthe following has relatively weak
evidence for benefit in treatment of pathological
gambling?
A. Gambling Anonymous
B. Behavioural therapy
C. Naltrexone
D. Acamprosate
E. N- Acetyl cysteine
Answer: Gambling Anonymous
MCQs
33.
Pathological gambling
Lottery,Roulette, Bingo and Gaming machines
Betting on sports like football, cricket, chess
Horse race
Casino’s
34.
Pathological gambling
Pathological Gambling-ICD 10
Frequent, repeated episodes of gambling which dominate the
individual's life to the detriment of social, occupational, material, and family values and commitments.
May put their jobs at risk, acquire large debts, and lie or break
the law to obtain money or evade payment of debts.
Intense urge to gamble, which is difficult to control, together with
preoccupation with ideas and images of the act of gambling and the circumstances that surround the act.
Preoccupations and urges often increase at times when life is
stressful
Also called "compulsive gambling" but this term is less
appropriate because the behaviour is not compulsive in the technical sense, nor is the disorder related to obsessive-
compulsive neurosis.
35.
Pathological gambling
Pathological Gambling– ICD 10
The essential feature of the disorder is persistently repeated
gambling, which continues and often increases despite adverse social consequences such as impoverishment, impaired
family relationships, and disruption of personal life.
Includes: compulsive gambling
Differential diagnosis. Pathological gambling should be
distinguished from: excessive gambling by manic patients;
gambling by sociopathic personalities
36.
[Renee M. Cunningham-Williamset al-2005]
Condition Percentage
NDS 38
ADS 26
GAD 19
Major depression 19
Binge eating 12
Prevalence & Psychiatric co morbidity
A total of 912 St. Louisians catchment area were interviewed.
Life time prevalence of PG was 2.5%
Sub threshold gamblers 12.4%
Recreational Gamblers 42.9%
Risk factors noticed were 18–20 years of age, unemployment,
having a novelty-seeking personality trait.
37.
Personality patterns..
Fourclinical personality patterns were the most
frequently identified
Antisocial
Obsessive-compulsive
Narcissistic
Dependent
Cluster analysis revealed two personality profiles
“antisocial profile" and "obsessive-compulsive
profile”
The "antisocial" group scores significantly higher on
all clinical syndromes
[Ortiz-Tallo M 2011]
Social Support
Individualswith lower levels of social support at
baseline had greater severity of problems in gambling,
psychiatric, and family domains
Social support plays an important role in moderating
treatment outcomes of pathological gamblers
[Nancy M. Petry 2009]
40.
Assessment Scales
Centrefor Addiction and Mental Health (CAMH):
Short Gambling Screen – 5 questions more than 2 yes
Lie or Bet screen – 2 questions
Problem Gambling Severity Index – 9 questions
41.
Psycho social interventions
CBGTvs MI
RCT compared individual MI [4 sessions] with CBGT with no
treatment group as control.
Both produced significant within-group decreases on most
outcome measures up to the 12-month follow-up & there was
no difference between them. [Per Carlbring et al.2009]
42.
Pharmacotherapy
Acamprosate 1998mg 65% has shown benefit
Donald W. Black 2011]
N Acetyl cysteine, 83.3% responded at the end of the
double-blind phase, compared with only 28.6% of those
assigned to placebo
[Grant JE 2007]
75% of subjects improved with Naltrexone upto
250mg/day compared to 24% of placebo group
[Kim SW, Grant JE,2001]
Pathological gambling ismore impulsive
38 subjects were assessed impulsivity, obsessionality and
compulsivity through questionnaire
Changes in PG-YBOCS scores after treatment correlated
with changes in Impulsiveness scores
Although PG exhibits features of both compulsivity and
Impulsivity but impulsivity predominates
Changes in gambling severity following treatment with
paroxetine was associated with changes in impulsivity
[Carlos Blanco et al.2009]
45.
Symptoms &diagnostic criteria.
Usually starts during adolescence.
Chronic, relapsing course.
Scores high on impulsivity.
Co morbid with externalizing behaviors.
5HT & Dopamine are involved.
Decreased functioning of vmPFC has been noticed.
Naltrexone has shown similar efficacy in treatment.
Pathological Gambling & Substance Use Disorder
(ADS)
Why addictive disorder?
46.
ICD 10 PathologicalFire setting (Pyromania)
Diagnostic guidelines
The essential features are:
(a) Repeated fire-setting without any obvious motive such as monetary
gain, revenge, or political extremism;
(b) Intense interest in watching fires burn; and
(c) Reported feelings of increasing tension before the act, and intense
excitement immediately after it has been carried out.
There may also be an abnormal interest in fire-engines and
other fire-fighting equipment, in other associations of fires,
and in calling out the fire service.
47.
Pyromania
61.9% hada current co morbid mood disorder.
47.6% met criteria for a current impulse-control disorder
[Grant E,Sukh won kim,2006]
3,965 students in grades 7 to 12 were surveyed.
Prevalence :once-27%, three or more time was 13%
Males> females, studying in high school
Low frequency fire setters more likely to report
psychological distress, binge drinking, frequent cannabis
use, and sensation seeking, delinquent behavior, suicidal
intent, and low parental monitoring [Sherri MacKay,2009]
48.
Pyromania
There areno standard treatments for pyromania.
Much of the literature on the use of psychological
treatments has focused on children and includes
behavioural therapies, family therapy, and fire
education.
Case reports have suggested benefit from SSRIs,
lithium, topiramate, olanzapine, and valproate.
[Grant, J.E., Odlaug, B.L. 2012]
49.
Kleptomania ICD 10
The term kleptomania was coined by the French psychiatrists
Esquirol and Marc in the 19th century.
Characterized by repeated failure to resist impulses to steal
objects that are not acquired for personal use or monetary
gain.
The objects may instead be discarded, given away, or
hoarded.
50.
Kleptomania ICD 10
Diagnosticguidelines
Increasing sense of tension before, and a sense of
gratification during and immediately after, the act.
Although some effort at concealment is usually made, not all
the opportunities for this are taken.
The theft is a solitary act, not carried out with an accomplice.
Anxiety, despondency, and guilt between episodes of
stealing from shops (or other premises) but this does not
prevent repetition.
51.
SSRI- Paroxetine,Fluvoxamine, Escitalopram has been
beneficial.
Naltrexone up to 145mg/day has shown 76% reduction in
urges over 3 years.
CBT treatments such as systematic desensitization, aversion
therapy, and covert sensitization have all been shown to have
benefit.
[Jon E Grant, Brian L Odlaug, 2008]
Kleptomania…Treatment
52.
Most effectivefirst line treatment for
Trichotillomania is
A. Aversion therapy
B. Habit Reversal Therapy
C. N Acetyl cysteine
D. Naltrexone
E. All of the above
Answer: Habit Reversal Therapy
MCQs
53.
Dermatitis paraartefectasyndrome includes
A. Skin picking
B. Nail biting
C. Trichotillomania (Hair pulling)
D. Self-harm by burning
E. None of the above
Answer: Trichotillomania (Hair pulling)
MCQs
54.
Trichotillomania
The wordis derived from the Greek
Thrix …..Hair
Tillein…..To pull
Mania ….Madness
2579 college students were studied for TTM, found a 0.6%
lifetime prevalence.
Hair pulling resulting in visible hair loss, but failing to
meet full criteria, was identified in 1.5% of males and
3.4% of females. [Christenson GA et al 1991]
Among 791 Israeli students of 17 years age lifetime
prevalence of TTM was 1%. [Robert A. King
1995]
55.
Typical three-phase zone
Zone 1: Long hair
(unremarkable, not affected,
normal hair/haircut).
Zone 2: Missing hair (recent
alopecia due to pulling).
Zone 3: Re growth of hair,
shorter and less regular than the
normal hair (older, former
alopecia areas with irregular hair
re growth after intermittent
pulling). [Clinical Management
in Psychodermatology byWolfgang Harth]
56.
Assessing Tools
TheMassachusetts General Hospital (MGH) Hair Pulling
Scale – Consists of 7 items each carrying up to 5 points
Trichotillomania Diagnostic Interview – 3 point clinician
rating for each DSM criteria.
National Institute of Mental Health Trichotillomania
Questionnaire – Derived from Y-BOCS consists of severity
& impairment scales.
Milwaukee Inventory of Subtypes of Trichotillomania:
adult version & children’s version – 7 Point scale
57.
Trichotillomania Trichotemnomania Trichoteiromania
Injury
pattern
Pullingout the
hair
Cutting off the
hair
Breaking off the
hair by
scratching
Clinical
findings
Typical three-
phase
configuration
Hair stubble that
appears shaved
Hair stubble
with
whitish-looking
ragged ends
Dermatitis Paraartefacta Syndrome
[Clinical Management in Psychodermatology by Wolfgang Harth]
58.
TTM & menstrualcycle
Premenstrual period- Exacerbation of actual hair pulling urge
intensity and frequency.
Ability to control pulling was alleviated during menstruation
and shortly thereafter.
[Keuthen et al 1997]
59.
Treatment of TTM
Psychotherapy
Habit reversal therapy ..most effective first line
treatment [van Minnen et al. 2003 ]
Acceptance & commitment therapy with HRT
[Woods et al.2006 ]
Cognitive Behavioural Therapy [Ninan PT 2000]
Pharmacotherapy
Naltrexone up to 50mg/day
[O’Sullivan, R.L., Christenson, G.A., 1999]
Olanzapine up to 10mg/day over 12 wk
[Van Ameringen M 2010]
N Acetyl cysteine. [Jon E. Grant, Brian L. Odlaug,2009]
60.
N-Acetyl cysteine
Ina 12-week, double-blind, placebo-controlled trial.
NAC on 50 patients with trichotillomania.
N- Acetyl Cysteine was dosed between 1200 and
2400mg/day.
Compared with controls, patients taking NAC experienced a
significant reduction in hair-pulling symptoms.
[Jon E. Grant, Brian L. Odlaug,2009]
61.
Skin picking [Psychogenicexcoriation]
Maladaptive skin excoriation or preoccupation with skin
excoriation and/or recurrent impulses to excoriate the skin
that is/are experienced as irresistible, intrusive, and/or
senseless, resulting in noticeable skin damage.
Associated with marked distress as they are time-consuming
& interfere with occupational activities.
Divided into compulsive, impulsive & mixed types.
[Arnold LM, Auchenbach MB, McElroy SL.2001]
62.
Skin picking
Prevalence: 2.04%.
[Calikusu C et al 2012]
Mean age of onset was 12.3+/-9.6yrs.
Face was the most common area.
Co morbidity Prevalence in %
Trichotillomania 36.7%.
Compulsive nail biting 26.7%
Depressive disorder 16.7%
Obsessive-compulsive
disorder
15%
[Odlaung BL, Grant JE 2008]
63.
Skin picking
Pharmacotherapy
Fluoxetine [Simeon D 1997]
Nonpharmacologic treatments
Habit reversal therapy
[Teng EJ 2006].
[Clinical Management in Psychodermatology byWolfgang Harth]
64.
Onychophagia
Boys Girls
ADHD 7868.2
ODD 39 31
Separation
anxiety
19.5 22.7
Tic disorder 17.1 4.5
OCD 14.6 4.5
Enuresis 24.4 0
Ahmad Ghanizadeh 2008
Chronic nail biting, Usually seen in children & young
adults decrease by 18 years of age.
Leads to severe damage to the cuticles and nails, paronychia and secondary bacterial infection, self-inflicted
gingival injuries, and dental problems.
65.
Compulsive sexual behavior
Excessive or uncontrolled sexual behavior(s)/ thoughts/
urges to engage in behavior and lead to significant distress,
social or occupational impairment, or legal and financial
consequences
[Brian L. Odlaug, Jon E. Grant 2010]
Co morbidity of 31% mood disorder, 33 % Anxiety disorder,
22 % of substance use disorder has been found.
Among ICD.
Kleptomania …14%
Pathological Gambling …11%
Compulsive buying …14% [Donald W. Black et al 1997]
66.
Compulsive sexual behaviourdisorder
Excessive sexual drive from the ICD-10 has been reclassified
in ICD-11 as Compulsive sexual behaviour disorder (CSBD,
6C72) and listed under Impulse control disorders.
Characterized by a persistent pattern of failure to control
intense, repetitive sexual impulses or urges resulting in
repetitive sexual behaviour.
Symptoms:
Repetitive sexual activities becoming a central focus of the
person’s life to the point of neglecting health and personal
care or other interests, activities and responsibilities;
numerous unsuccessful efforts to significantly reduce
repetitive sexual behaviour; and
Continued repetitive sexual behaviour despite adverse
consequences or deriving little or no satisfaction from it.
67.
The patternof failure to control intense, sexual impulses or
urges and resulting repetitive sexual behaviour is manifested
over an extended period of time (e.g., 6 months or more),
and causes marked distress or significant impairment in
personal, family, social, educational, occupational, or other
important areas of functioning.
Distress that is entirely related to moral judgments and
disapproval about sexual impulses, urges, or behaviours is
not sufficient to meet this requirement.
Compulsive sexual behaviour disorder
68.
No standardtreatment available.
Imaginal desensitization, aversion therapy, group therapy
and psychodynamic psychotherapy.
Treatment- SSRI, Medroxyprogesterone Acetate
[Victoria L. Codispoti,2008]
69.
Repeated aggressiveacts that result in assault or
destruction of property in disproportion to stimulus.
2,554 adults, life time prevalence was 5.8%, 12 month
prevalence of 4.1%.
Unemployment was the major risk factor.
[Alexander N. Ortega et al.-2008]
Treatment - lithium, anticonvulsants (Phenytoin,
Valproic acid, Carbamazapine, Topiramate), SSRI,
Lower dose of newer antipsychotics, CBT, Contingency
management.
Intermittent Explosive Disorder
Gaming disorder
Gamingdisorder (6C51) has been newly added to the ICD-
11, and placed in the group "Disorders due to addictive
behaviours", alongside Gambling disorder (6C50).
Aside from Gaming disorder, the ICD-11 also features
Hazardous gaming (QE22), an ancillary category used to
identify problematic gaming which does not rise to the level
of a disorder.
The DSM-5 (2013) features a similar category called Internet
Gaming Disorder (IGD).
Problematic internet use
Is it a new independent psychiatric disorder?
Is certain individuals having problematic Internet use in
relation to specific online activities?[Video games, Porn,
Social network]
Young(1998) selected eight of the 10 gambling criteria as
diagnostic criteria.
Treatment
Cognitive-behavioral therapy [Davis, 2001]
Education and training [Young & Case, 2004]
74.
Compulsive shopping
Initiallyrecognized by Kraepline & Bleuler as
ONIOMANIA.
Uncontrollable.
Markedly distressing.
Time-consuming, and/or resulting in family, social,
vocational, and/or financial difficulties.
Prevalence between 5.8%. [Koran et al 2006]
CBT is shown to be effective . [Mitchell JE 2006]
75.
Food Addiction
AQualitative Internet Study was conducted from 2000 to 10
29,406 unique users, aged 8 to 21
were assessed using modified
DSM 4 substance dependence
criteria
29% reported that they were
addicted to food
[Robert A Pretlow 2011]
Prevalence ranges from
11% to 25%
When studied with Yale food
addiction questionnaire
[Adrian Meule, Marco Diana, 2011]
Symptom Percentage
Tolerance 77%
Withdrawal 56%
Intense cravings 46%
Weight Prevalence
Underweight 10
Normal-weight 6.3
Overweight 14
Obese 37.5
76.
Exercise addiction
Exerciseaddiction has to be distinguished from exercise
done with high frequency and intensity
Defined according to modified DSM criteria for
substance dependence
Prevalence : 3%
Eating disorder : 39-48%
Exercise tends to cluster with food disorders, caffeine use,
and shopping
[Marilyn Freimuth 2011]
77.
Conclusion
Relationship betweenImpulsivity & compulsivity are intricate.
These symptoms overlap in many psychiatric disorders
Limited studies on epidemiology at present. There exists
tremendous scope for research in this direction
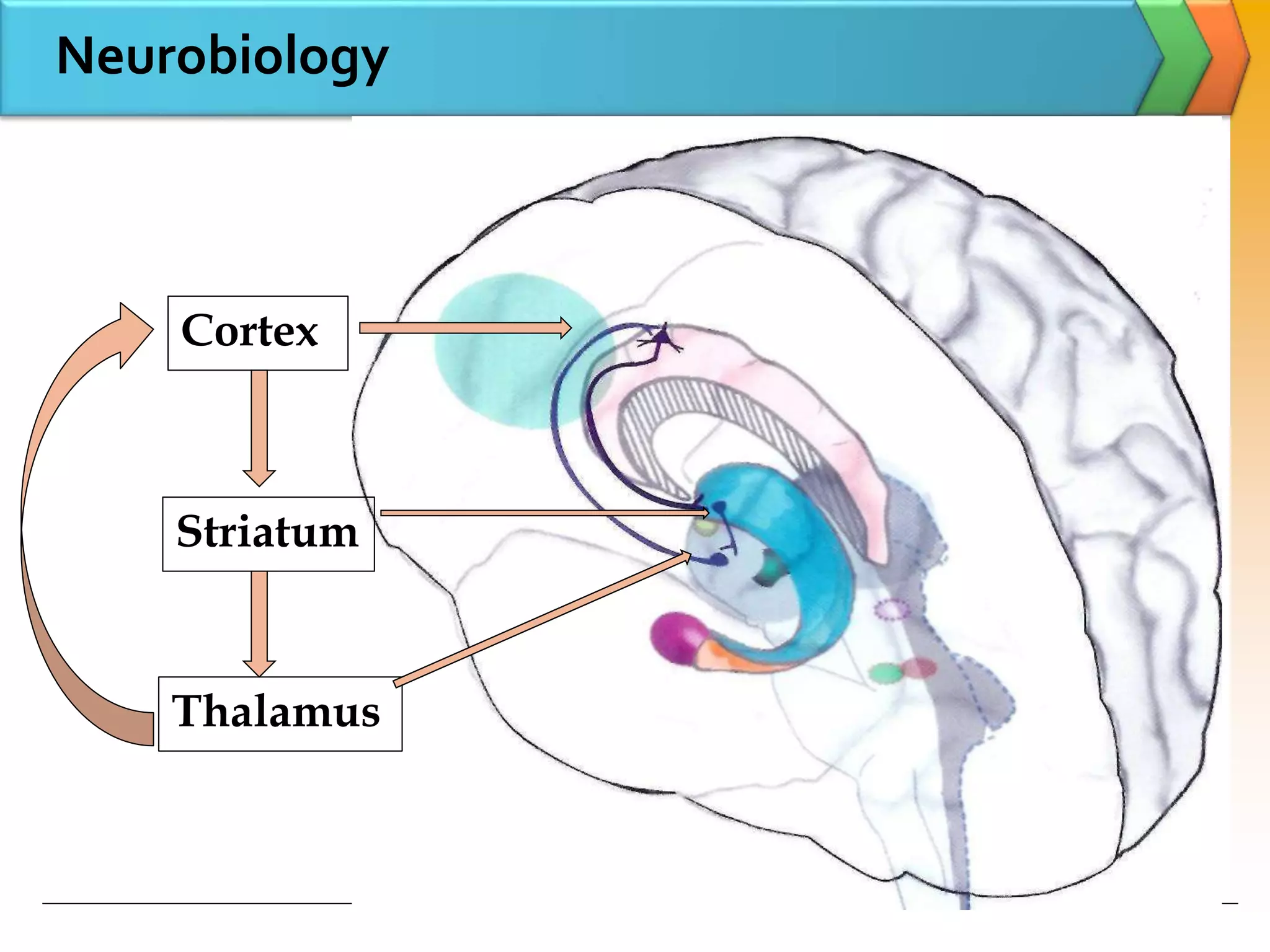
Evidence in neurobiology shows involvement of reward
pathway including vmPFC, OFC, Striatum[ventral to dorsum]
in all ICD similar to substance use disorder
N-Acetyl- Cysteine – new molecule shows promise in
managing TTM, the research findings need to be
communicated to mental health providers
78.
Conclusion
TTM, skinpicking resemble OC related disorders, but
Pathological gambling, other newer additions like
compulsive sexual behavior, compulsive buying, internet
addiction, food addiction, exercise addiction resemble
substance use disorder- reflecting the progress in
understanding of these conditions.
Proposed changes in ICD 11 and DSM 5 reflects the better
understanding and progress in research among these conditions
Hence to include TTM & skin picking in OC related disorder
To include IED by DSM 5 - in disruptive, impulse & conduct
disorder
Pathological gambling by DSM 5- in ‘Substance & Addictive
Disorder.’
79.
Conclusion
Newer BehavioralAddictions need more time and
work to understand, conduct epidemiological studies
and only then consider them in the classificatory system,
hence tremendous potential for research in this area.
![What is Impulsivity?
Rapid, unplanned reactions to stimuli before complete
processing of information.
Decreased sensitivity to negative consequences of behavior.
Lack of regard for long-term consequences.
Impulsivity often has an impact, not only on the impulsive
individual, but also on others.
[F. Gerard Moeller, Ernest S. Barratt,2001]
Failure to inhibit behaviors motivated by reward.
[Grant et al.2006]](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-4-2048.jpg)
![What is Compulsivity?
Failure to suppress repetitive behaviors designed to relieve
tension or reduce a negative emotion state.
[Grant et al.2006]
Desire to avoid harm.
[Fineberg et al., 2010]](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-6-2048.jpg)




![ICD-10 Habit and Impulse Disorder
F63.0 Pathological gambling
F63.1 Pathological fire-setting [pyromania]
F63.2 Pathological stealing [kleptomania]
F63.3 Trichotillomania
F63.8 Other habit and impulse disorders
F63.9 Habit and impulse disorder, unspecified
ICD 10](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-13-2048.jpg)

![Prevalence in general population
791 students were screened for ICD.
Prevalence of one lifetime ICD was 10.4%,two was 1.5%.
[Brian L. Odlaug 2010]
Disorder Prevalence in
percentage
Trichotillomania 3.92
Compulsive sexual behavior 3.67
Compulsive buying 1 .90
Pyromania 1.01
Pathological gambling 0.63
Intermittent explosive disorder 0.51
Kleptomania 0.38](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-19-2048.jpg)

![ICD among Parkinson's disease
Around 3000 PD patients interviewed for ICD
More common in patients treated with a dopamine agonist
than in patients not taking a dopamine agonist [odds ratio:2.72]
[Daniel Weintraub 2010]
Prevalence in %
Any ICD 13.6
Pathological Gambling 5
Compulsive sexual behavior 3.5
Compulsive buying 5.7
Binge eating 4.3](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-21-2048.jpg)


![ Incentive sensitization theory-repeated drug exposure leads
to a sensitization (reverse tolerance) of the incentive-
motivational properties of behavior and behavior-related
cues, where NAcc & Dopamine role has been implicated
Opponent process theory-the first involves affective or
hedonic habituation, the second process is an affective or
hedonic withdrawal
Neuroplasticity theory- contributing to addiction is the
recruitment of habit-based neurocircuitry throughout
repeated drug exposure
[Christopher M. Olsen 2011]
Theories of behavioral plasticity & addiction](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-24-2048.jpg)





![[Renee M. Cunningham-Williams et al-2005]
Condition Percentage
NDS 38
ADS 26
GAD 19
Major depression 19
Binge eating 12
Prevalence & Psychiatric co morbidity
A total of 912 St. Louisians catchment area were interviewed.
Life time prevalence of PG was 2.5%
Sub threshold gamblers 12.4%
Recreational Gamblers 42.9%
Risk factors noticed were 18–20 years of age, unemployment,
having a novelty-seeking personality trait.](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-36-2048.jpg)
![Personality patterns..
Four clinical personality patterns were the most
frequently identified
Antisocial
Obsessive-compulsive
Narcissistic
Dependent
Cluster analysis revealed two personality profiles
“antisocial profile" and "obsessive-compulsive
profile”
The "antisocial" group scores significantly higher on
all clinical syndromes
[Ortiz-Tallo M 2011]](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-37-2048.jpg)
![Pathways of Pathological gambling
Ecological Factors
Classical & operant
conditioning
Habituation
Chasing
Pathological gambling
Emotional
vulnerability
Biological
vulnerability
Impulsivity
Traits
[Alex Blaszczynski 2006]](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-38-2048.jpg)
![Social Support
Individuals with lower levels of social support at
baseline had greater severity of problems in gambling,
psychiatric, and family domains
Social support plays an important role in moderating
treatment outcomes of pathological gamblers
[Nancy M. Petry 2009]](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-39-2048.jpg)

![Psycho social interventions
CBGT vs MI
RCT compared individual MI [4 sessions] with CBGT with no
treatment group as control.
Both produced significant within-group decreases on most
outcome measures up to the 12-month follow-up & there was
no difference between them. [Per Carlbring et al.2009]](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-41-2048.jpg)
![Pharmacotherapy
Acamprosate 1998 mg 65% has shown benefit
Donald W. Black 2011]
N Acetyl cysteine, 83.3% responded at the end of the
double-blind phase, compared with only 28.6% of those
assigned to placebo
[Grant JE 2007]
75% of subjects improved with Naltrexone upto
250mg/day compared to 24% of placebo group
[Kim SW, Grant JE,2001]](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-42-2048.jpg)

![Pathological gambling is more impulsive
38 subjects were assessed impulsivity, obsessionality and
compulsivity through questionnaire
Changes in PG-YBOCS scores after treatment correlated
with changes in Impulsiveness scores
Although PG exhibits features of both compulsivity and
Impulsivity but impulsivity predominates
Changes in gambling severity following treatment with
paroxetine was associated with changes in impulsivity
[Carlos Blanco et al.2009]](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-44-2048.jpg)
![Pyromania
61.9% had a current co morbid mood disorder.
47.6% met criteria for a current impulse-control disorder
[Grant E,Sukh won kim,2006]
3,965 students in grades 7 to 12 were surveyed.
Prevalence :once-27%, three or more time was 13%
Males> females, studying in high school
Low frequency fire setters more likely to report
psychological distress, binge drinking, frequent cannabis
use, and sensation seeking, delinquent behavior, suicidal
intent, and low parental monitoring [Sherri MacKay,2009]](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-47-2048.jpg)
![Pyromania
There are no standard treatments for pyromania.
Much of the literature on the use of psychological
treatments has focused on children and includes
behavioural therapies, family therapy, and fire
education.
Case reports have suggested benefit from SSRIs,
lithium, topiramate, olanzapine, and valproate.
[Grant, J.E., Odlaug, B.L. 2012]](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-48-2048.jpg)

![ SSRI- Paroxetine, Fluvoxamine, Escitalopram has been
beneficial.
Naltrexone up to 145mg/day has shown 76% reduction in
urges over 3 years.
CBT treatments such as systematic desensitization, aversion
therapy, and covert sensitization have all been shown to have
benefit.
[Jon E Grant, Brian L Odlaug, 2008]
Kleptomania…Treatment](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-51-2048.jpg)
![Trichotillomania
The word is derived from the Greek
Thrix …..Hair
Tillein…..To pull
Mania ….Madness
2579 college students were studied for TTM, found a 0.6%
lifetime prevalence.
Hair pulling resulting in visible hair loss, but failing to
meet full criteria, was identified in 1.5% of males and
3.4% of females. [Christenson GA et al 1991]
Among 791 Israeli students of 17 years age lifetime
prevalence of TTM was 1%. [Robert A. King
1995]](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-54-2048.jpg)
![Typical three-phase zone
Zone 1: Long hair
(unremarkable, not affected,
normal hair/haircut).
Zone 2: Missing hair (recent
alopecia due to pulling).
Zone 3: Re growth of hair,
shorter and less regular than the
normal hair (older, former
alopecia areas with irregular hair
re growth after intermittent
pulling). [Clinical Management
in Psychodermatology byWolfgang Harth]](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-55-2048.jpg)

![Trichotillomania Trichotemnomania Trichoteiromania
Injury
pattern
Pulling out the
hair
Cutting off the
hair
Breaking off the
hair by
scratching
Clinical
findings
Typical three-
phase
configuration
Hair stubble that
appears shaved
Hair stubble
with
whitish-looking
ragged ends
Dermatitis Paraartefacta Syndrome
[Clinical Management in Psychodermatology by Wolfgang Harth]](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-57-2048.jpg)
![TTM & menstrual cycle
Premenstrual period- Exacerbation of actual hair pulling urge
intensity and frequency.
Ability to control pulling was alleviated during menstruation
and shortly thereafter.
[Keuthen et al 1997]](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-58-2048.jpg)
![Treatment of TTM
Psychotherapy
Habit reversal therapy ..most effective first line
treatment [van Minnen et al. 2003 ]
Acceptance & commitment therapy with HRT
[Woods et al.2006 ]
Cognitive Behavioural Therapy [Ninan PT 2000]
Pharmacotherapy
Naltrexone up to 50mg/day
[O’Sullivan, R.L., Christenson, G.A., 1999]
Olanzapine up to 10mg/day over 12 wk
[Van Ameringen M 2010]
N Acetyl cysteine. [Jon E. Grant, Brian L. Odlaug,2009]](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-59-2048.jpg)
![N-Acetyl cysteine
In a 12-week, double-blind, placebo-controlled trial.
NAC on 50 patients with trichotillomania.
N- Acetyl Cysteine was dosed between 1200 and
2400mg/day.
Compared with controls, patients taking NAC experienced a
significant reduction in hair-pulling symptoms.
[Jon E. Grant, Brian L. Odlaug,2009]](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-60-2048.jpg)
![Skin picking [Psychogenic excoriation]
Maladaptive skin excoriation or preoccupation with skin
excoriation and/or recurrent impulses to excoriate the skin
that is/are experienced as irresistible, intrusive, and/or
senseless, resulting in noticeable skin damage.
Associated with marked distress as they are time-consuming
& interfere with occupational activities.
Divided into compulsive, impulsive & mixed types.
[Arnold LM, Auchenbach MB, McElroy SL.2001]](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-61-2048.jpg)
![Skin picking
Prevalence : 2.04%.
[Calikusu C et al 2012]
Mean age of onset was 12.3+/-9.6yrs.
Face was the most common area.
Co morbidity Prevalence in %
Trichotillomania 36.7%.
Compulsive nail biting 26.7%
Depressive disorder 16.7%
Obsessive-compulsive
disorder
15%
[Odlaung BL, Grant JE 2008]](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-62-2048.jpg)
![Skin picking
Pharmacotherapy
Fluoxetine [Simeon D 1997]
Nonpharmacologic treatments
Habit reversal therapy
[Teng EJ 2006].
[Clinical Management in Psychodermatology byWolfgang Harth]](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-63-2048.jpg)

![Compulsive sexual behavior
Excessive or uncontrolled sexual behavior(s)/ thoughts/
urges to engage in behavior and lead to significant distress,
social or occupational impairment, or legal and financial
consequences
[Brian L. Odlaug, Jon E. Grant 2010]
Co morbidity of 31% mood disorder, 33 % Anxiety disorder,
22 % of substance use disorder has been found.
Among ICD.
Kleptomania …14%
Pathological Gambling …11%
Compulsive buying …14% [Donald W. Black et al 1997]](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-65-2048.jpg)


![ No standard treatment available.
Imaginal desensitization, aversion therapy, group therapy
and psychodynamic psychotherapy.
Treatment- SSRI, Medroxyprogesterone Acetate
[Victoria L. Codispoti,2008]](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-68-2048.jpg)
![ Repeated aggressive acts that result in assault or
destruction of property in disproportion to stimulus.
2,554 adults, life time prevalence was 5.8%, 12 month
prevalence of 4.1%.
Unemployment was the major risk factor.
[Alexander N. Ortega et al.-2008]
Treatment - lithium, anticonvulsants (Phenytoin,
Valproic acid, Carbamazapine, Topiramate), SSRI,
Lower dose of newer antipsychotics, CBT, Contingency
management.
Intermittent Explosive Disorder](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-69-2048.jpg)



![Problematic internet use
Is it a new independent psychiatric disorder?
Is certain individuals having problematic Internet use in
relation to specific online activities?[Video games, Porn,
Social network]
Young(1998) selected eight of the 10 gambling criteria as
diagnostic criteria.
Treatment
Cognitive-behavioral therapy [Davis, 2001]
Education and training [Young & Case, 2004]](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-73-2048.jpg)
![Compulsive shopping
Initially recognized by Kraepline & Bleuler as
ONIOMANIA.
Uncontrollable.
Markedly distressing.
Time-consuming, and/or resulting in family, social,
vocational, and/or financial difficulties.
Prevalence between 5.8%. [Koran et al 2006]
CBT is shown to be effective . [Mitchell JE 2006]](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-74-2048.jpg)
![Food Addiction
A Qualitative Internet Study was conducted from 2000 to 10
29,406 unique users, aged 8 to 21
were assessed using modified
DSM 4 substance dependence
criteria
29% reported that they were
addicted to food
[Robert A Pretlow 2011]
Prevalence ranges from
11% to 25%
When studied with Yale food
addiction questionnaire
[Adrian Meule, Marco Diana, 2011]
Symptom Percentage
Tolerance 77%
Withdrawal 56%
Intense cravings 46%
Weight Prevalence
Underweight 10
Normal-weight 6.3
Overweight 14
Obese 37.5](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-75-2048.jpg)
![Exercise addiction
Exercise addiction has to be distinguished from exercise
done with high frequency and intensity
Defined according to modified DSM criteria for
substance dependence
Prevalence : 3%
Eating disorder : 39-48%
Exercise tends to cluster with food disorders, caffeine use,
and shopping
[Marilyn Freimuth 2011]](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-76-2048.jpg)
![Conclusion
Relationship between Impulsivity & compulsivity are intricate.
These symptoms overlap in many psychiatric disorders
Limited studies on epidemiology at present. There exists
tremendous scope for research in this direction
Evidence in neurobiology shows involvement of reward
pathway including vmPFC, OFC, Striatum[ventral to dorsum]
in all ICD similar to substance use disorder
N-Acetyl- Cysteine – new molecule shows promise in
managing TTM, the research findings need to be
communicated to mental health providers](https://image.slidesharecdn.com/impulsecontroldisorderkapil1-211216231048/75/Impulse-control-disorder-77-2048.jpg)































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)

















