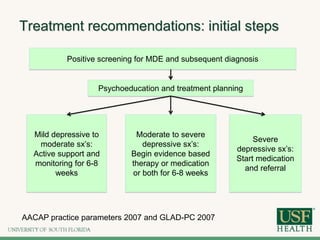
This document discusses the treatment of depression in children and adolescents. It covers symptoms of depression, diagnostic criteria, course of illness, common comorbidities, treatment options including psychotherapy and medication management. Psychoeducation is recommended for all patients, while mild cases may only require supportive care. Moderate to severe depression is often treated with evidence-based therapies such as CBT or medication in addition to psychoeducation. The goals of treatment are response, remission, and recovery from depressive symptoms.