
Recommended
More Related Content
What's hot
What's hot (20)
Similar to GOUT SOAP FORMAT CASE PRESNTATION.
Similar to GOUT SOAP FORMAT CASE PRESNTATION. (20)
More from varshawadnere
More from varshawadnere (20)
Recently uploaded
Recently uploaded (20)
GOUT SOAP FORMAT CASE PRESNTATION.
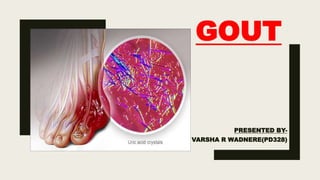
- 1. GOUT PRESENTED BY- VARSHA R WADNERE(PD328)
- 2. ■ GOUT-metabolic disorder of purine metabolism. ■ CAUSES: Excess uric acid, excess purine diet, inability of kidneys to flush out uric acid, defective purine metabolism, urate crystals, alcohol consumption. ■ SIGNS AND SYMPTOMS OF GOUT: Intense pain, swelling, warm in joint,tendernes, tophi, inflammation.
- 3. S0AP ANALYSIS PATIENT DETAILS: ■ NAME- MR.GRAND ■ AGE- 55yrs ■ SEX- MALE ■ WEIGHT-94.5kg ■ Height-179cm ■ BMI-30(OVERWEIGHT)
- 4. SUBJECTIVE DATA ■ PAIN,SWELLING AND REDNESS IN HIS RIGHT GREAT TOE. ■ WOKE UP IN NIGHT WITH EXTREME EXCRUCIATING PAIN IN TOE,BY MORNING HIS TOE WAS DARK RED AND WARM. ■ SAME EPISODE WAS FACED BY HIM 3yrs Ago.
- 6. ASSESSMENT ■ PROVISIONAL DIAGNOSIS: FOOT PAIN,EFFUSION OF FOOT PAIN ■ FINAL DIAGNOSIS: GOUT
- 7. HISTORY ■ MAJOR CHILDHOOD ILLNESS- DENIES RHEUMATIC OR SCARLET FEVER,MUMPS,PERTUSIS. ■ ADULTHOOD ILLNESS- HYPERTENSION,HYPERLIPIDEMIA. ■ MEDICATION: HYDROCHLOROTHIAZIDE 25MG DAILY, DILTIAZEM CD 300MG DAILY. ■ ALLERGIES: ACE INHIBITORS. ■ FAMILY HISTORY: FATHER DIED DUE TO COMPLICATION DIABETES AND HYPERTENSION AND BROTHER HAVE HYPERTENSION. ■ 3-4 BEER CONSUMPTION DAILY AT NIGHT.
- 8. GOALS OF TREATMENT ■ The three general goals of therapy in the management of gout recommended by British Society of Rheumatology: ■ Management of the acute painful attack ■ Recommendations to change diet, lifestyle modifications and implementation non-pharmacological modalities. ■ Management of recurrent or chronic gout
- 9. ASSESSMENT OF CURRENT THERAPY 1. Indomethacin (50mg- 3 times/day.) • INDICATION: NSAIDs. • ADR:VERTIGO, DYSPEPSIA, POSTOPERATIVE HEMORRHAGE . • CONTRAINDICATIONS:ASTHMA, GI DISEASE, HYPERKALEMIA. • INTERACTIONS: DIGOXIN,VANCOMYCIN, PHENYLBUTAZONE.
- 10. 2. ALLOPURINOL(300MG-OD) • INDICATION: XANTHINE OXIDASE INHIBITOR USED FOR PRIMARYAND SECONARYGOUT. • ADR: RENAL FAILURE SYNDROME, APLASTICANEMIA, PANCREATITIS. • CONTRAINDICATION: LESCH NYHAN SYNDROME, USE OF DIDANOSINE • INTERACTIONS:WARFARIN, CICLOSPORIN,AZATHIOPRINE.
- 11. PLANNING ■ Mr. Grand is asked to follow-up in 3 months. At this visit routine lab work will be done. ■ He is advised to follow-up if he has an attack before his next visit. ■ If any drug doesn’t work or condition get worse contact physician to change the drug therapy.
- 12. POINT TO PHYSICIAN ■ FOR HYPERTENSION HYDROCHLORTHIAZIDE WAS GIVEN BUT THAT DRUG WORSE THE CONDITION OF GOUT SO INSTEAD OF THAT CALCIUM CHANNEL BLOCKER SHOULD PRESCRIBED.
- 13. POINT TO PATIENT ■ Keep a supply of NSAIDS and take it as soon as first symptoms appear. ■ Reduce weight. ■ Reduce alcohol consumption. ■ Avoid daily intake of organ meat, especially liver. ■ Drink plenty of water preferably 10-12 glasses per day. ■ Regular follow-up at 3-month intervals ■ Report if acute attacks are frequent, not responding to NSAIDS, or if systemic features develop. ■ Should avoid purine-rich foods (such as beer, some fish, and spinach), and reduce their total calorie intake and cholesterol intake. ■ Pain area should be rested and use of ice may help. ■ If dose is missed do not take double dose.
- 14. REFERENCES ■ GOUT CASE STUDY- essentiavite1.com ■ India drug index
- 15. ANY QUESTONS?