Downloaded 88 times



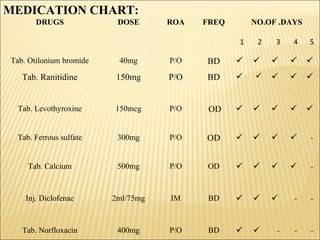





A 45-year-old female patient presented with facial puffiness, myalgia, increased tiredness, hoarseness of voice and headache. Lab investigations revealed hypothyroidism. She was diagnosed with hypothyroidism and prescribed levothyroxine, otilonium bromide, ranitidine, ferrous sulfate, and calcium. The pharmacist intervened to recommend changing the dosing interval between levothyroxine and calcium to 4 hours apart to maximize levothyroxine efficacy and monitoring serum TSH levels.










































































