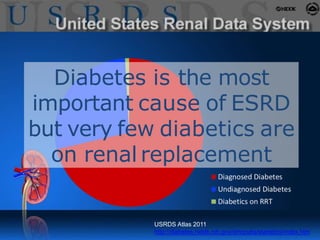
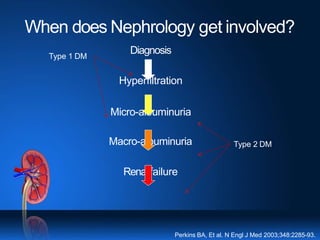
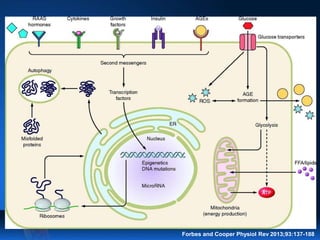
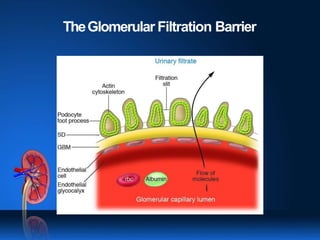
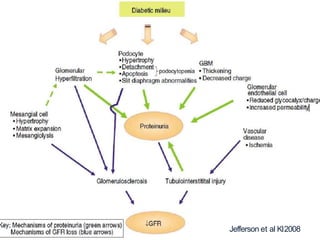
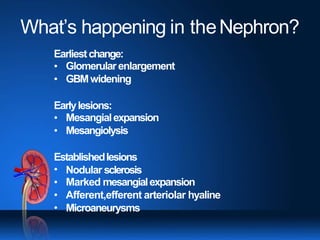
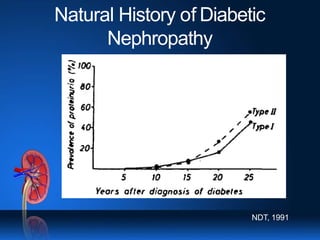
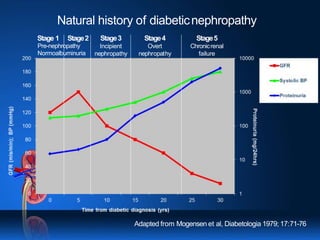
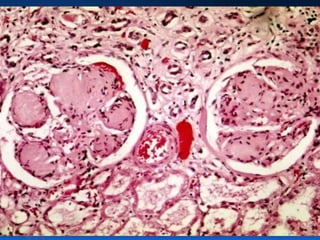
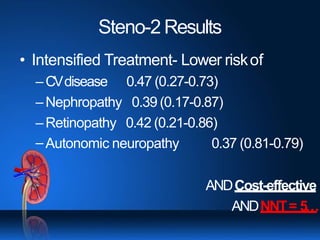
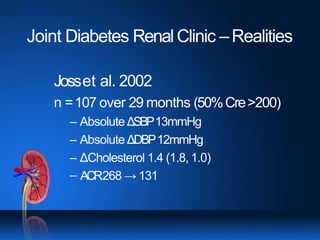
This document discusses diabetic kidney disease and its treatment. It notes that diabetes is a leading cause of end-stage renal disease and places a large burden on healthcare systems. The pathogenesis of diabetic nephropathy involves changes to the glomerular filtration barrier that lead to proteinuria and declining kidney function over time if not treated. Treatment focuses on tight control of blood glucose, blood pressure, cholesterol, and RAAS inhibitors to slow progression of kidney disease and reduce cardiovascular risk. An integrated treatment approach targeting multiple risk factors simultaneously can significantly reduce complications compared to conventional treatment.