Downloaded 171 times

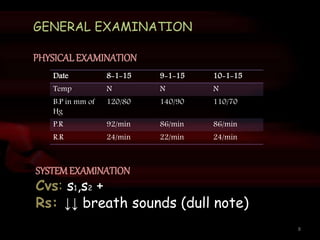
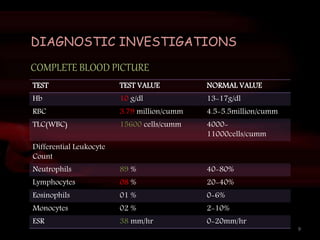
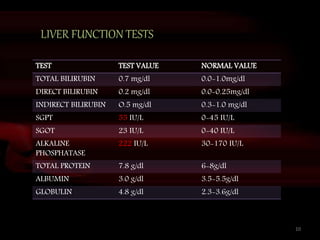
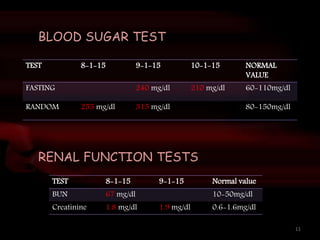
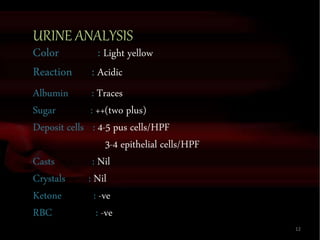
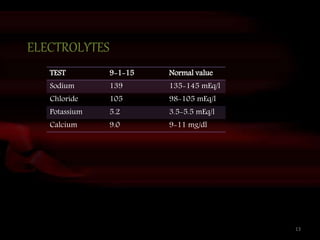

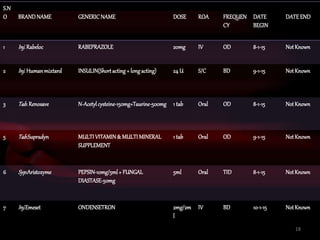
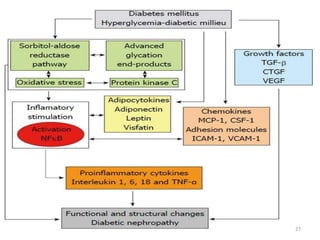



This document presents a case study of a 50-year-old male patient with chronic kidney disease due to diabetic nephropathy. The patient has a 15-year history of type 2 diabetes and non-proliferative diabetic retinopathy. Diagnostic tests show elevated blood sugar, creatinine, and signs of kidney damage. The patient is assessed as having progressed chronic kidney disease due to diabetic nephropathy. His treatment plan includes insulin, medications to protect the kidneys and manage symptoms, and lifestyle changes to control his diabetes and slow disease progression.























































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)











