Glaucoma
• Bahar Ghorbani
•MSc student
• Faculty Of Rehabilitation Sciences , Iran University Of Medical Sciences
• Baharghorbani424@gmail.com
2.
Definitions
• Glaucoma isa group of diseases characterized by optic nerve damage,
optic disc changes, and distinct patterns of visual dysfunction. While
elevated intraocular pressure (IOP) is a major risk factor, it is not
essential for defining the disease. In most cases, optic nerve damage and
visual field loss are influenced by IOP levels and the nerve's resistance to
damage. Some glaucoma patients have normal IOP, but factors like
corneal thickness and diurnal IOP variations may affect measurements.
Treatment typically focuses on lowering IOP, but in some cases, optic
nerve damage may continue despite IOP reduction due to other
pathological mechanisms.
3.
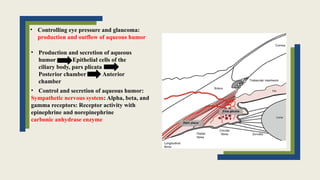
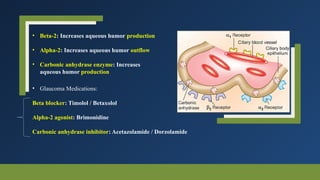
• Controlling eyepressure and glaucoma:
production and outflow of aqueous humor
• Production and secretion of aqueous
humor Epithelial cells of the
ciliary body, pars plicata
Posterior chamber Anterior
chamber
• Control and secretion of aqueous humor:
Sympathetic nervous system: Alpha, beta, and
gamma receptors: Receptor activity with
epinephrine and norepinephrine
carbonic anhydrase enzyme
4.
Aqueous humor formationand secretion into the posterior chamber result from the
following:
• active secretion, which takes place in the double-layered ciliary epithelium
• ultrafiltration
• simple diffusion
Active secretion requires energy to transport substances against an electrochemical gradient and
is independent of pressure. While the exact ions involved are unclear, sodium, chloride, and
bicarbonate play a role. This process, primarily responsible for aqueous humor production,
partially depends on carbonic anhydrase II.
Ultrafiltration is a pressure-dependent movement of fluid influenced by hydrostatic pressure
favoring inflow and oncotic pressure resisting it. The exact relationship between secretion and
ultrafiltration is unknown.
Diffusion is the passive movement of ions across membranes based on charge and concentration.
Aqueous humor contains higher hydrogen and chloride ions and lower bicarbonate than plasma.
It is virtually protein-free, maintaining optical clarity. Components include growth factors,
enzymes (carbonic anhydrase, lysozyme, etc.), prostaglandins, cAMP, catecholamines, steroid
hormones, and hyaluronic acid. The production rate is 2.0–2.5 µL/min, and its composition
changes as it flows through the posterior chamber, pupil, and anterior chamber.
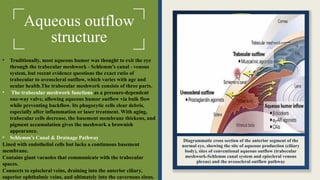
Diagrammatic cross sectionof the anterior segment of the
normal eye, showing the site of aqueous production (ciliary
body), sites of conventional aqueous outflow (trabecular
meshwork-Schlemm canal system and episcleral venous
plexus) and the uveoscleral outflow pathway
• Traditionally, most aqueous humor was thought to exit the eye
through the trabecular meshwork - Schlemm’s canal - venous
system, but recent evidence questions the exact ratio of
trabecular to uveoscleral outflow, which varies with age and
ocular health.The trabecular meshwork consists of three parts.
• The trabecular meshwork functions as a pressure-dependent
one-way valve, allowing aqueous humor outflow via bulk flow
while preventing backflow. Its phagocytic cells clear debris,
especially after inflammation or laser treatment. With aging,
trabecular cells decrease, the basement membrane thickens, and
pigment accumulation gives the meshwork a brownish
appearance.
• Schlemm’s Canal & Drainage Pathway
Lined with endothelial cells but lacks a continuous basement
membrane.
Contains giant vacuoles that communicate with the trabecular
spaces.
Connects to episcleral veins, draining into the anterior ciliary,
superior ophthalmic veins, and ultimately into the cavernous sinus.
Aqueous outflow
structure
7.
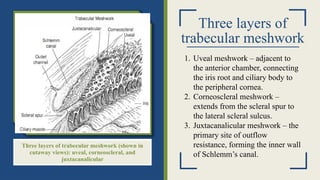
Three layers of
trabecularmeshwork
Three layers of trabecular meshwork (shown in
cutaway views): uveal, corneoscleral, and
juxtacanalicular
1. Uveal meshwork – adjacent to
the anterior chamber, connecting
the iris root and ciliary body to
the peripheral cornea.
2. Corneoscleral meshwork –
extends from the scleral spur to
the lateral scleral sulcus.
3. Juxtacanalicular meshwork – the
primary site of outflow
resistance, forming the inner wall
of Schlemm’s canal.
8.
Aqueous outflow
structure
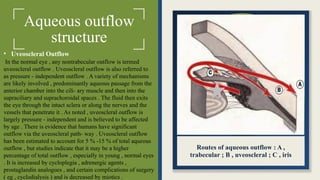
• UveoscleralOutflow
In the normal eye , any nontrabecular outflow is termed
uveoscleral outflow . Uveoscleral outflow is also referred to
as pressure - independent outflow . A variety of mechanisms
are likely involved , predominantly aqueous passage from the
anterior chamber into the cili- ary muscle and then into the
supraciliary and suprachoroidal spaces . The fluid then exits
the eye through the intact sclera or along the nerves and the
vessels that penetrate it . As noted , uveoscleral outflow is
largely pressure - independent and is believed to be affected
by age . There is evidence that humans have significant
outflow via the uveoscleral path- way . Uveoscleral outflow
has been estimated to account for 5 % -15 % of total aqueous
outflow , but studies indicate that it may be a higher
percentage of total outflow , especially in young , normal eyes
. It is increased by cycloplegia , adrenergic agents ,
prostaglandin analogues , and certain complications of surgery
( eg , cyclodialysis ) and is decreased by miotics .
Routes of aqueous outflow : A ,
trabecular ; B , uveoscleral ; C , iris
9.
Distribution of IOPin the Population and Its Relation to Glaucoma
Epidemiological studies show that the mean intraocular pressure (IOP) is around 15.5 mmHg, with a
standard deviation of 2.6 mmHg. The distribution is non-Gaussian, skewed toward higher pressures,
especially in individuals over 40. The traditional threshold of 21 mmHg for defining abnormal
pressure is flawed, as glaucoma can occur at lower pressures, and some individuals tolerate higher
IOP without damage. While IOP is a key risk factor for glaucoma, it is not the sole determinant, and
its modification remains the only effective intervention.
Factors Influencing IOP
IOP fluctuates due to factors such as time of day, heartbeat, respiration, exercise, fluid intake, and
medications. Alcohol temporarily lowers IOP, whereas cannabis reduces it but is not clinically
viable due to short duration and side effects. IOP is generally higher when lying down due to
increased episcleral venous pressure and tends to rise with age, with genetic predisposition playing a
role.
Diurnal Variation
IOP varies 2-6 mmHg throughout the day, with fluctuations greater than 10 mmHg indicating
potential glaucoma. Peak pressures typically occur in the early morning, often while still in bed.
Continuous monitoring of IOP outside clinic hours can help explain optic nerve damage despite
seemingly controlled pressure. Systemic hypotension, especially during sleep, may contribute to
optic nerve damage by reducing blood flow.
10.
Anatomy and
Pathology ofthe
Optic Nerve
The optic nerve connects the retina to the brain, consisting of
about 1.2–1.5 million retinal ganglion cell (RGC) axons. It has
anterior and posterior segments, expanding in size after exiting
the eye due to axonal myelination and glial tissue. There are
three major RGC types: M cells (motion-sensitive, low-light
adaptation), P cells (color vision, fine detail processing), and
bistratified cells (blue-yellow color opponency). The superior
and inferior nerve fibers are more vulnerable to glaucoma,
leading to characteristic visual field defects. The anterior optic
nerve has four layers: nerve fiber, prelaminar, laminar, and
retrolaminar. The lamina cribrosa supports the optic nerve as it
exits the eye and may play a role in glaucoma-related damage.
Blood supply primarily comes from branches of the ophthalmic
artery, mainly the short posterior ciliary arteries. The vascular
network is interconnected, while venous drainage mainly occurs
through the central retinal vein.
Anterior optic nerve vasculature. A, Arterial supply to the anterior optic
nerve and peripapillary choroid. Lamina cribrosa (LC), superficial nerve
fiber layer (NFL), prelamina (PL), retrolamina (RL), central retinal artery
(CRA), optic nerve (ON), choroid (C), posterior ciliary artery (PCA),
retina (R), sclera (S). B, Venous drainage of the anterior optic nerve and
peripapillary choroid. Lamina cribrosa (LC), nerve fiber layer (NFL),
prelamina (PL), retrolamina (RL), choroid (C), retina (R), sclera (S), optic
nerve (ON), central retinal vein (CRV).
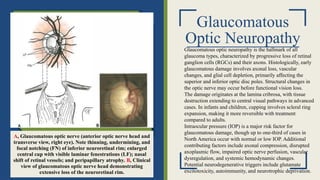
11.
Glaucomatous
Optic Neuropathy
A, Glaucomatousoptic nerve (anterior optic nerve head and
transverse view, right eye). Note thinning, undermining, and
focal notching (FN) of inferior neuroretinal rim; enlarged
central cup with visible laminar fenestrations (LF); nasal
shift of retinal vessels; and peripapillary atrophy. B, Clinical
view of glaucomatous optic nerve head demonstrating
extensive loss of the neuroretinal rim.
Glaucomatous optic neuropathy is the hallmark of all
glaucoma types, characterized by progressive loss of retinal
ganglion cells (RGCs) and their axons. Histologically, early
glaucomatous damage involves axonal loss, vascular
changes, and glial cell depletion, primarily affecting the
superior and inferior optic disc poles. Structural changes in
the optic nerve may occur before functional vision loss.
The damage originates at the lamina cribrosa, with tissue
destruction extending to central visual pathways in advanced
cases. In infants and children, cupping involves scleral ring
expansion, making it more reversible with treatment
compared to adults.
Intraocular pressure (IOP) is a major risk factor for
glaucomatous damage, though up to one-third of cases in
North America occur with normal or low IOP. Additional
contributing factors include axonal compression, disrupted
axoplasmic flow, impaired optic nerve perfusion, vascular
dysregulation, and systemic hemodynamic changes.
Potential neurodegenerative triggers include glutamate
excitotoxicity, autoimmunity, and neurotrophic deprivation.
12.
Neural degeneration inglaucoma may have a number of
triggers:
1. Hypotension & Reduced Ocular Blood Flow
• Systemic hypotension, vasospasms, and nocturnal BP dips reduce optic nerve perfusion.
• Fluctuations in ocular perfusion pressure cause oxidative stress and neurodegeneration.
2. Oxidative Stress & Mitochondrial Dysfunction
• Increased ROS and mitochondrial damage lead to retinal ganglion cell (RGC) apoptosis.
3. Glutamate Toxicity & Excitotoxicity
• Excess glutamate overstimulates NMDA receptors, increasing calcium influx and triggering
apoptosis.
4. Inflammation & Blood-Retina Barrier Dysfunction
• Chronic inflammation (elevated TNF-α, IL-6, and microglial activation) contributes to axonal
degeneration.
5. Mechanical Susceptibility of the Optic Nerve Head
• Weaker lamina cribrosa in some patients increases susceptibility to axonal compression and
impaired axoplasmic flow, leading to nerve damage.
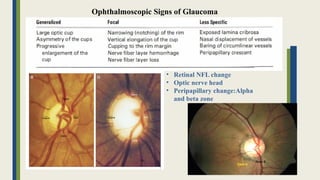
13.
Ophthalmoscopic Signs ofGlaucoma
• Retinal NFL change
• Optic nerve head
• Peripapillary change:Alpha
and beta zone
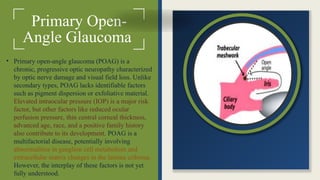
Primary Open-
Angle Glaucoma
•Primary open-angle glaucoma (POAG) is a
chronic, progressive optic neuropathy characterized
by optic nerve damage and visual field loss. Unlike
secondary types, POAG lacks identifiable factors
such as pigment dispersion or exfoliative material.
Elevated intraocular pressure (IOP) is a major risk
factor, but other factors like reduced ocular
perfusion pressure, thin central corneal thickness,
advanced age, race, and a positive family history
also contribute to its development. POAG is a
multifactorial disease, potentially involving
abnormalities in ganglion cell metabolism and
extracellular matrix changes in the lamina cribrosa.
However, the interplay of these factors is not yet
fully understood.
16.
POAG is usuallyinsidious in onset, slowly progressive, and painless. Though usually
bilateral, it can be quite asymmetric. Because central vision is relatively unaffected until
late in the disease, visual field loss, as measured by standard automated perimetry, may be
severe before symptoms are noted. POAG is diagnosed by assessment of the optic disc
appearance and the visual field.
• Direct mechanical damage
• Ischaemic damage
Normal-tension glaucoma (NTG)
Juvenile open-angle glaucoma (JOAG) Ocular hypertension
Glaucoma suspect
Topical medications (first-line treatment)
Laser trabeculoplasty
Glaucoma filtering surgery
Antifibrotic agents (Mitomycin C or 5-Fluorouracil)
Incisional surgery (for low baseline IOP cases)
Non-β-blocker medications (for IOP ≤15 mmHg)
17.
Primary Risk Factors:
1.Age:
Higher prevalence with increasing age, especially in Black individuals (11% in those 80+ years).
Visual field defects progress 7 times more in patients aged 60+ compared to those under 40.
Age is an independent risk factor, even without increased intraocular pressure (IOP).
2. Race:
POAG is 3-4 times more common in Black and Hispanic individuals than in non-Hispanic Whites.
Black patients are more likely to be diagnosed at a younger age and at an advanced stage.
3. Family History:
A person with a sibling with POAG has a 3.7-fold increased risk.
Associated Disorders:
1. Myopia:
Strongly associated with POAG; high myopia increases glaucoma risk.
Diagnosing POAG is more difficult in highly myopic eyes due to optic disc abnormalities.
2. Diabetes Mellitus:
Some studies show an association, while others do not.
OHTS found diabetes may reduce glaucoma risk, though selection bias may have influenced results.
3. Blood Pressure:
Hypertension: May lower glaucoma risk in younger individuals but increase it in older ones.
Low Ocular Perfusion Pressure: Strongly linked to glaucoma development.
Overtreatment of hypertension may worsen glaucoma progression.
4. Retinal Vein Occlusion (RVO):
Patients with RVO may have preexisting POAG.
Glaucoma and ocular hypertension (OHT) are risk factors for central RVO.
5. Other Conditions:
Sleep apnea, thyroid disorders, hypercholesterolemia, migraine, and Raynaud’s phenomenon may be linked to POAG, but further
research is needed.
18.
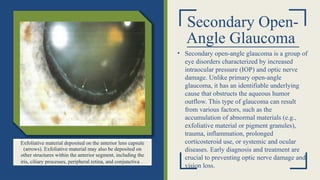
Secondary Open-
Angle Glaucoma
•Secondary open-angle glaucoma is a group of
eye disorders characterized by increased
intraocular pressure (IOP) and optic nerve
damage. Unlike primary open-angle
glaucoma, it has an identifiable underlying
cause that obstructs the aqueous humor
outflow. This type of glaucoma can result
from various factors, such as the
accumulation of abnormal materials (e.g.,
exfoliative material or pigment granules),
trauma, inflammation, prolonged
corticosteroid use, or systemic and ocular
diseases. Early diagnosis and treatment are
crucial to preventing optic nerve damage and
vision loss.
Exfoliative material deposited on the anterior lens capsule
(arrows). Exfoliative material may also be deposited on
other structures within the anterior segment, including the
iris, ciliary processes, peripheral retina, and conjunctiva .
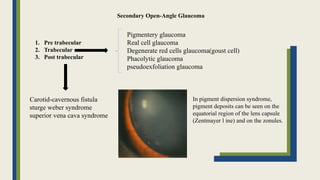
19.
1. Pre trabecular
2.Trabecular
3. Post trabecular
Pigmentery glaucoma
Real cell glaucoma
Degenerate red cells glaucoma(goust cell)
Phacolytic glaucoma
pseudoexfoliation glaucoma
Carotid-cavernous fistula
sturge weber syndrome
superior vena cava syndrome
In pigment dispersion syndrome,
pigment deposits can be seen on the
equatorial region of the lens capsule
(Zentmayer l ine) and on the zonules.
Secondary Open-Angle Glaucoma
20.
Risk factors forsecondary open-angle glaucoma include:
1. Advanced age – The risk increases with age.
2. Family history – Having a close relative with glaucoma raises the likelihood of developing the
disease.
3. Prolonged corticosteroid use – Especially steroid-containing eye drops.
4. Associated ocular conditions – Such as Pigmentary Dispersion Syndrome and Exfoliation
Syndrome.
5. Intraocular inflammation (uveitis) – Can lead to obstruction of aqueous humor outflow.
6. Eye trauma and previous surgeries – Injuries or intraocular surgeries may contribute to
increased intraocular pressure (IOP).
7. Diabetes and vascular diseases – Can affect the blood flow to the optic nerve.
8. High myopia (nearsightedness) – In some cases, it is linked to an increased risk of secondary
open-angle glaucoma.
9. Low blood pressure or circulatory disorders – May reduce blood supply to the optic nerve.
10. Systemic diseases like Marfan syndrome or hereditary neuropathies – Could be associated
with this type of glaucoma.
21.
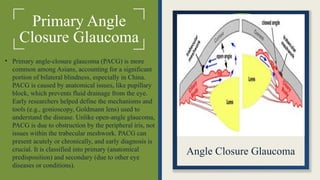
Primary Angle
Closure Glaucoma
•Primary angle-closure glaucoma (PACG) is more
common among Asians, accounting for a significant
portion of bilateral blindness, especially in China.
PACG is caused by anatomical issues, like pupillary
block, which prevents fluid drainage from the eye.
Early researchers helped define the mechanisms and
tools (e.g., gonioscopy, Goldmann lens) used to
understand the disease. Unlike open-angle glaucoma,
PACG is due to obstruction by the peripheral iris, not
issues within the trabecular meshwork. PACG can
present acutely or chronically, and early diagnosis is
crucial. It is classified into primary (anatomical
predisposition) and secondary (due to other eye
diseases or conditions).
Angle Closure Glaucoma
22.
Pathophysiology of AngleClosure
Pupillary Block
Pupillary block is the most common cause of angle closure, especially in primary angle-closure
glaucoma (PACG). It occurs when aqueous humor flow is obstructed at the lens-iris interface,
creating a pressure difference that pushes the peripheral iris forward against the trabecular
meshwork. This blockage is most severe when the pupil is mid-dilated. In rare cases, complete
pupillary block happens due to 360° posterior synechiae. It can involve contact with the natural
lens, intraocular lens, capsular remnants, or vitreous substances like silicone oil. A peripheral
iridectomy can relieve the blockage.
Underlying Mechanisms of Angle Closure
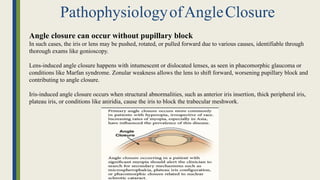
23.
Angle closure canoccur without pupillary block
In such cases, the iris or lens may be pushed, rotated, or pulled forward due to various causes, identifiable through
thorough exams like gonioscopy.
Lens-induced angle closure happens with intumescent or dislocated lenses, as seen in phacomorphic glaucoma or
conditions like Marfan syndrome. Zonular weakness allows the lens to shift forward, worsening pupillary block and
contributing to angle closure.
Iris-induced angle closure occurs when structural abnormalities, such as anterior iris insertion, thick peripheral iris,
plateau iris, or conditions like aniridia, cause the iris to block the trabecular meshwork.
PathophysiologyofAngleClosure
24.
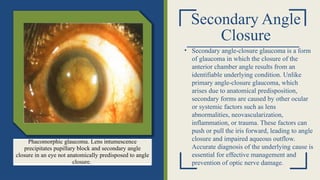
Secondary Angle
Closure
• Secondaryangle-closure glaucoma is a form
of glaucoma in which the closure of the
anterior chamber angle results from an
identifiable underlying condition. Unlike
primary angle-closure glaucoma, which
arises due to anatomical predisposition,
secondary forms are caused by other ocular
or systemic factors such as lens
abnormalities, neovascularization,
inflammation, or trauma. These factors can
push or pull the iris forward, leading to angle
closure and impaired aqueous outflow.
Accurate diagnosis of the underlying cause is
essential for effective management and
prevention of optic nerve damage.
Phacomorphic glaucoma. Lens intumescence
precipitates pupillary block and secondary angle
closure in an eye not anatomically predisposed to angle
closure.
25.
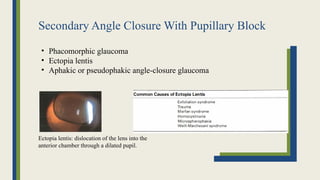
Secondary Angle ClosureWith Pupillary Block
• Phacomorphic glaucoma
• Ectopia lentis
• Aphakic or pseudophakic angle-closure glaucoma
Ectopia lentis: dislocation of the lens into the
anterior chamber through a dilated pupil.
26.
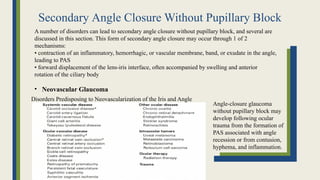
Secondary Angle ClosureWithout Pupillary Block
A number of disorders can lead to secondary angle closure without pupillary block, and several are
discussed in this section. This form of secondary angle closure may occur through 1 of 2
mechanisms:
• contraction of an inflammatory, hemorrhagic, or vascular membrane, band, or exudate in the angle,
leading to PAS
• forward displacement of the lens-iris interface, often accompanied by swelling and anterior
rotation of the ciliary body
• Neovascular Glaucoma
Disorders Predisposing to Neovascularization of the Iris and Angle
Angle-closure glaucoma
without pupillary block may
develop following ocular
trauma from the formation of
PAS associated with angle
recession or from contusion,
hyphema, and inflammation.
27.
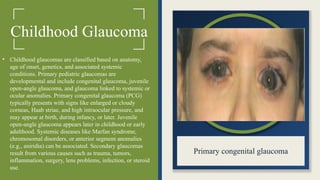
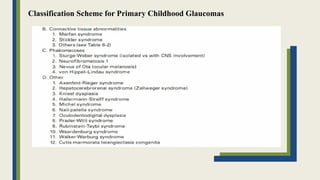
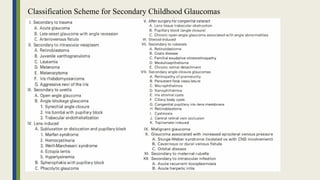
Childhood Glaucoma
• Childhoodglaucomas are classified based on anatomy,
age of onset, genetics, and associated systemic
conditions. Primary pediatric glaucomas are
developmental and include congenital glaucoma, juvenile
open-angle glaucoma, and glaucoma linked to systemic or
ocular anomalies. Primary congenital glaucoma (PCG)
typically presents with signs like enlarged or cloudy
corneas, Haab striae, and high intraocular pressure, and
may appear at birth, during infancy, or later. Juvenile
open-angle glaucoma appears later in childhood or early
adulthood. Systemic diseases like Marfan syndrome,
chromosomal disorders, or anterior segment anomalies
(e.g., aniridia) can be associated. Secondary glaucomas
result from various causes such as trauma, tumors,
inflammation, surgery, lens problems, infection, or steroid
use.
Primary congenital glaucoma


































![Polymer [ बहुलक ] Chemistry Notes PDF - Irfanullah Mehar - JJ Sir Chemistry.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/polymerchemistrynotespdf-irfanullahmehar-jjsirchemistry-260210172118-3f9b37f7-thumbnail.jpg?width=640&height=640&fit=bounds)


















