Download to read offline
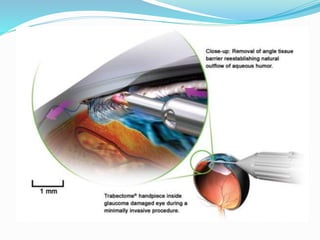



Ab interno trabeculectomy (AIT) using the trabectome is a minimally invasive surgical technique for managing glaucoma by improving aqueous drainage and reducing intraocular pressure. The procedure requires only a small incision, preserving the conjunctiva, and features a favorable safety profile compared to traditional methods. Developed in the early 2000s, the trabectome has gained FDA clearance and is used for treating both adult and infantile glaucoma.

























































![Glaucoma drainage devices[1]](https://cdn.slidesharecdn.com/ss_thumbnails/glaucomadrainagedevices1-170104084412-thumbnail.jpg?width=640&height=640&fit=bounds)




































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)












