Diathermy
Diathermy has ahand control (or foot pad) and a patient
adhesive ground plate (patient return electrode) which is
typically placed on a large well-perfused muscle, eg. the
thigh.
Is a device used for heating of the body tissues by the
passage of high frequency electrical current which results
in coagulation, desiccation or cutting of tissues.
Monopolar diathermy is used for both surgical
dissection as a bloodless knife and for hemostasis
Monopolar Diathermy is not used for circumcision, brain
surgery, plastic surgery, and ophthalmology cases
because of the danger is coagulation of blood vessels (eg.
the dorsal artery of the penis) which may result in
ischemia and necrosis of the involved tissues.
7.
Diathermy
Complications of diathermyinclude:
1. Mild thermal injury (burns)
2. Damage to adjacent tissues
3. Increased susceptibility to infection and
seromas
4. Burns at areas of attachment of ECG pads if
the grounding plate is not properly attached
5. Damage to ischemic tissues & ischemia.
Contraindications – persons with pacemakers.
9.
Nasogastric Tube
Closedactive or passive drain
Its uses are diagnostic and therapeutic
Diagnostic uses include: diagnosing the presence and
amount of blood in the stomach.
Therapeutic uses include:
1. decompression of the stomach
2. removal of activated charcoal given to children in acute
poisoning
3. nutritional (administration of enteral feeds)
4. administration of drugs
10.
Nasogastric (NG) Tube
Contraindications:
1. Basal skull fracture as evidenced by CSF otorrhea or
rhinorrhea, Battle’s sign (mastoid ecchymosis), or Raccoon
eyes (periorbital ecchymosis). CSF is confirmed by the ring
sign is by placing a drop of the bloody drainage on a piece of
filter paper, and looking for the Ring Sign. This is the
appearance of a yellow ring around the periphery of the drop
of blood.
2. Facial fractures.
The alternative to the nasogastric tube is the orogastric tube
which is placed orally using the McGill’s forceps.
Complication includes malplacement into the trachea which
may result in pulmonary aspiration and abscess.
12.
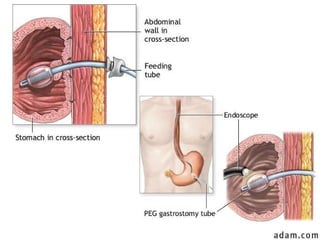
Gastrostomy Tube
• Whatis gastrostomy feeding tube
placement?
Gastrostomy feeding tube placement is a
procedure in which the surgeon creates an
alternate entrance into the stomach. A tube is
placed through the abdominal wall directly into
the stomach, bypassing the mouth and
esophagus. When done at the time of an
operation it is called open gastrostomy tube
placement. When performed with the aid of a
lighted flexible scope it is called Percutaneous
Endoscopic Gastrostomy tube insertion (or
PEG).
13.
Gastrostomy Tube
• Gastrostomyfeeding may be indicated for patients
with a functioning gastrointestinal tract who require
long term tube feeding. This includes patients in
whom malnutrition already exists, or may result,
secondary to:
• neurologic diseases resulting in an abnormality in swallowing.
• tumors of the head, neck, or esophagus resulting in an
abnormality in swallowing.
• upper airway diseases/mouth, throat, or neck trauma
resulting in an abnormality in swallowing.
• In addition, some patients who require either chronic
supplemental fluids for hydration or chronic gastric
decompression are candidates for gastrostomy tube
placement.
14.
Gastrostomy Tube
• Gastrostomytubes allow for decompression of
the stomach to prevent vomiting or aspiration
pneumonia.
• What happens during the procedure?
Gastrostomy feeding tube placement is done in two
basic ways. In the first, open gastrostomy tube
placement is generally performed under general
anesthesia. This procedure is often done at the
time of another major operation in anticipation of
postoperative need for emptying (decompressing)
the stomach, or for future feeding.
15.
Gastrostomy Tube
•The secondway, called percutaneous
endoscopic gastrostomy (PEG) tube
placement is usually done with IV sedation
and a local anesthetic applied to the back
of the mouth. The procedure is done with
the guidance of an endoscope placed
through the patient’s mouth into their
stomach.
•OPEN TECHNIQUE: The gastrostomy tube
is placed through a small cut in the
abdominal wall and into the stomach. A
balloon on the end of the tube is inflated
inside the stomach.
16.
Gastrostomy Tube
• Tractionis placed on the tube to elevate the
stomach against the abdominal wall where it is
secured with sutures. Sometimes a second
smaller tube is threaded through the stomach
tube into the first part of the intestine. This is
called a jejunostomy tube and is used to feed or
administer medications to patients further down
the gastrointestinal tract beyond the stomach.
This smaller tube may reduce the risk of
regurgitation or reflux of contents into the
stomach, esophagus, and lung. Following the
tube placement the abdominal wall incision is
closed and the patient is taken to the recovery
room.
17.
Tube Gastrostomy
Gastrostomy TubeCare
I. Dressing Changes (every 1 to 2 days)
a) Clean around tube with hydrogen peroxide.
b) Apply antibiotic ointment to skin around tube.
c) Dress with gauze pads and tape.
d) Position tube so it does not kink.
II. Showers - no tub baths.
a) Cover dressing with a double layer of plastic wrap and tape
edges.
b) Remove plastic wrap and change dressing after you shower
III. Activities - no specific restrictions.
18.
Tube Gastrostomy
IV. Feeding
a)Use water to flush the tube after each feeding.
b) Use liquid forms of medication if possible.
c) Ask your doctor or nurse to provide you with specific information
about feedings or medications.
V. Possible problems that can arise with your tube.
a) Leakage of feedings around the tube.
b) Signs of infection such as swelling, tenderness, redness, or drainage
of pus around the tube.
c) If the tube falls out completely call immediately. The tube usually can
be easily replaced if it is done within 24 hours from the time it fell
out. Waiting longer could mean that a separate new tube will have to
be placed.
Flatus Tube
Large flexiblerubber tube
Placed into the rectum in patients with sigmoid
volvulus and for pseudo-colonic obstruction
Requirements:
Protective covering
Disposable flatus tube and connection tubing
Bowl of tepid water (into which the non-lubricated end
goes)
Lubricant
Disposable wipes
Disposable gloves
Complications: perforation of bowel in patient’s with
impaired sensation eg spinally injured patients
24.
Fleet Enema
•Is aphosho-sodium enema
•Is an osmotically active agent
•Used for clearing/preparing bowel eg. For left sided
bowel resection and anastomosis, IVP or lower GI
endoscopy.
•Complications:
• Elderly persons can get fluid and electrolyte imbalance,
therefore avoid in old patients and those with cardiac and
kidney problems
25.
Metronidazole 500 mg
•Antimicrobial agent
• Is used prophylactically or therapeutically for coverage
of anaerobes.
• Prophylactically it is administered 15 mg/kg IV 30 mins
prior to bowel resection / colorectal surgery (maximum
dose 1g/dose); then 7.5 mg/kg IV q6h x 2
• Ceftriaxone is co-administered for coverage of aerobes
(eg. Gram-negatives and gram-positives).
• Therapeutic doses are used if there is established
infection (15 mg/kg IV, then 7.5 mg/kg q6h
maximum = 1g/dose)
27.
Colostomy Bag
• Acolostomy is an artificial opening made in the large bowel to divert
feces and flatus to the exterior, where it can be collected in an
external appliance
• Types:
• Temporary vs Permanent
• Trans-sigmoidal vs Transverse vs Sigmoid
28.
Colostomy
•A temporary (loop)colostomy is most commonly
established to defunction an anastomosis after an
anterior resection, to prevent fecal peritonitis
developing following traumatic injury to the rectum
or colon, and to facilitate the operative treatment
of a high fistula in ano. Eg. Hartman’s procedure.
Most loop colostomies are made in the transverse
colon but the sigmoid colon can be suitable.
29.
Colostomy
•A double-barrelled colostomyis another type of
temporary colostomy in which the colon is divided
so that both ends can be brought separately to the
surface, ensuring that the distal segment is
completely defunctioned.
•A permanent (end) colostomy is formed by bringing
the distal end of the divided colon to the surface in
the left iliac fossa, where it is sutured in place
joining the colonic margin to the surrounding skin.
30.
Complications of Colostomy
•Prolapse
•Retraction
•Necrosisof the distal end
•Stenosis of the orifice
•Colostomy hernia
•Bleeding (usu from granulomas around the margin of
the colostomy)
•Colostomy diarrhea
Many of these complications require revision of the colostomy.
32.
Sigmoidoscopy
•Flexible sigmoidoscopy enablesthe physician to look at
the inside of the large intestine from the rectum
through the sigmoid or descending colon.
•It may be done to find the cause of diarrhea,
abdominal pain, or constipation. It may also be done to
look for early signs of cancer in the descending colon
and rectum.
•With flexible sigmoidoscopy, the physician can see
bleeding, inflammation, abnormal growths, and ulcers
in the descending colon and rectum.
33.
Sigmoidoscopy
• If anythingunusual is in the rectum or colon, like a polyp or inflamed
tissue, the physician can remove a piece of it using instruments inserted
into the scope. The physician will send that piece of tissue (biopsy) to the
lab for testing.
• The bowel must be properly prepared by giving an enema and ensuring
an empty stomach.
• Hemorrhage and puncture of the colon are possible complications of
sigmoidoscopy.
Sutures: Catgut
• Plain(Catgut) Suture
Natural (causes a greater tissue reaction than vicryl)
Absorbable by enzymatic activity
Used for approximation of the edges of a surgical wound, blood vessels,
fat
Maintains its strength for < 7 days
• Catgut (chromic)
Natural (causes a greater tissue reaction than vicryl)
Absorbable by enzymatic activity
Used for approximating the edges of wounds of the lips, mucous
membranes and other tissues that heal slowly.
Also used in ophthalmology and in ligature of blood vessels.
Maintains its strength for 7-14 days (the chromium coating prolongs
strength)
38.
Sutures for SmallBowel
Silk
Natural
Non absorbable
Multi-filamentous
Has memory
Is smooth and passes thru the tissues easily
Used for bowel anastomosis (outer layer), ligation,
scalp and skin approximation in most body tissues,
ophthalmology, plastic surgery.
T-tube
Closed, passive drain(attaches to a drainage bag)
Comes in different sizes
One end inserts into the common bile duct, the
opposite end inserts into the common hepatic duct,
and the remaining end into the cystic duct
Used for drainage of bile in patients with biliary
leak after common bile duct exploration
Advantages: Decompression of the biliary system;
formation of tract for radiologic instrumentation
and stone removal
43.
T-tube
•This is atube placed in the common bile duct with
an ascending and descending limb that forms a “T”
•Drains percutaneously allows free drainage and
passage of small stones.
•It is usually placed after common bile duct
exploration or post cholecystectomy.
•It is usually removed after 3/52. It may be
removed if the bilirubin level does not increase and
there are no signs and symptoms of cholangitis
after clamping and after a normal T-tube
cholangiogram.
44.
T-tube
•After removal ofa T-tube the bile duct does not
leak bile because a fibrous tract forms around the
T-tube prior to removal. The fibrous tract then
scleroses down after removal of the T-tube,
resulting in a patent and closed bile duct.
•Complications:
• Bile Peritonitis
• Obstruction of the tube
• Displacement of the tube
• Ascending infection
46.
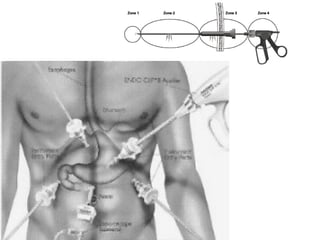
Laparoscopic Surgery
• Laparoscopicsurgery utilizes a high-resolution video
camera and a few customized instruments, to allow the
surgeon to perform surgery with minimal tissue injury and
manipulation. The camera and instruments are inserted
thru various ports inserted thru small incisions.
• Minimally invasive Laparoscopic surgery often results in the
following advantages over conventional incisions:
• Less post operative pain
• Less complications
• Shorter recovery period
• Earlier return to work
• Smaller incisions
• Better cosmetic result
47.
Laparoscopic Surgery
• LaparoscopicCholecystectomy
• Laparoscopic hernia repairs
• Laparoscopic colon surgery
• Laparoscopic gastric fundoplication
• Laparoscopic spleenectomy
• Laparoscopic intestinal surgery
• Laparoscopic Hiatal hernia surgery
• Surgical weight loss procedures:
(VBG) vertical banded gastroplasty
Roux-en-Y gastric bypass
• Laparoscopic appendectomy
49.
Sengstaken Blakemore Tube
Thistube is used for mechanical tamponade of
variceal hemorrhage. It consists of 2 balloons and is
placed nasally into the stomach. When its position in
the stomach has been confirmed radiographically, the
distal gastric balloon is inflated with 250 ml of air,
drawn tight against the GE junction, and placed on
traction. If the gastric balloon alone does not control
the hemorrhage, the proximal esophageal balloon is
inflated to a pressure of 20 mmHg.
50.
Sengstaken Blakemore Tube
Balloon tamponade is a temporary measure to control
bleeding and can be applied for 12-24 hours. 50% of
patients re-bleed after balloon deflation.
Risks include esophageal perforation and necrosis of
esophageal mucosa from overinflation of the balloon.
Other methods of arresting hemorrhage include:
1. Banding
2. Sclerotherapy
3. Transjugular intrahepatic portosystemic shunt (TIPS)
4. Shunt surgery
5. Octreotide/Vasopressin
6. Linton Ballon (has no gastric balloon)
52.
Mousseau Barbin Tube
•Used for palliation in a patient with non-resectable esophageal CA
• It does not contract, therefore aspiration is a risk when the patient
lies down.
• It lasts for 6-12 months before it becomes occluded
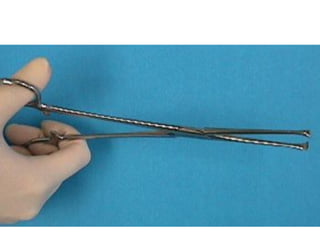
Breast Surgery: Allis
•An Allis is used to grasp tissue eg. subcutaneous fascia.
• Available in short and long sizes. A "Judd-Allis" holds intestinal
tissue; a "heavy Allis" holds breast tissue.
• Used in hernia repair, breast surgery
58.
Hemostat
•A hemostat isused to clamp small blood vessels or
tag sutures. Its jaws may be straight or curved.
Other names: crile, snap or stat.
60.
Core needle biopsy
•This procedure is similar to fine needle
aspiration, but the needle is larger, enabling a
larger sample to be obtained. It is performed
under local anesthesia and ultrasound or
stereotactic mammography is used if the lump
cannot be felt.
• Three to six needle insertions are needed to
obtain an adequate sample of tissue. A clicking
sound may be heard as the samples are being
taken and the patient may feel some pressure,
but should not feel pain. The procedure takes a
few minutes and no stitches are required.
61.
Tru-Cut Biopsy:
• Coreneedle biopsy may provide a more
accurate analysis and diagnosis than fine
needle aspiration because tissue is removed,
rather than just cells. This procedure is not
accurate in patients with very small or hard
lumps.
• Needle procedures are performed in doctors’
offices, clinics, surgical centers, and hospitals.
Informed consent is needed.
• Complications are rare, but excessive swelling,
redness, and bleeding or other drainage can
indicate an infection or abnormal bleeding.
62.
Breast Biopsy: Types
TruCut Needle Biopsy
•Tru Cut Needle Biopsy is also done in the office, usually
requires local anesthesia and takes a larger sample of
tissue. This needle is more often used for a large
palpable mass.
Fine Needle Aspiration
•Fine needle aspiration is probably the most expedient
method. It is generally performed in the office, and
diagnostic accuracy approaches 100%. The false
negative rate is 2-10%. However, a negative result
does not exclude cancer.
63.
Breast Biopsy: Types
IncisionalBiopsy
•Incisional biopsy involves removing only a sample of
tissue surgically from a very large mass for diagnostic
purposes. This is performed in an operating room.
Excisional Biopsy
•Excisional biopsy is the term used to describe removal
of the entire mass. This type of biopsy is performed in
an operating room under local or general anesthesia.
65.
Sutures for BreastSurgery
• Catgut for approximating subcutaneous tissues
• Vicryl repede
Synthetic (non-dye)
Absorbable
Used for skin closure especially when doing a subcuticular stitch.
Maintains strength for up to 14 days (strength shorter because there is no
dye)
67.
Hemovac Drain
Is anactive closed drain
Because it is closed there is less likely to be
secondary infection
It has a clear, collapsible drum-type reservoir
therefore there is the advantage that the fluid
collection can be directly observed. There are
gradations on the side so that volume can easily be
measured.
Used for drainage of abdominal abscess cavities,
breast abscess cavities, pelvic and others.
69.
Penrose Drain
Is afloppy cylinder of latex rubber; is flat.
Open, passive drain
Evacuates fluid by capillary action
Uses
Breast flap
Foot flap
Areas in the abdomen where there was an abscess
Post thyroidectomy
May be used for drainage of the abdominal abscess cavities and
esp. after bladder or kidney surgery.
Advantages: simple, inexpensive, and promotes the
development of a well-established tract within 7-10 days
Disadvantages: requires a relatively large skin incision, there
is increased risk of infection with use, and is not very effective
in emptying a cavity
71.
Chest Tube withTrochar
•Chest Tube Closed active or passive drain
It is used for the drainage of blood, fluid, chyle or air
from the thoracic cavity, as well as for the restoration of
negative pressure in the thoracic cavity and hence re-
expansion of the lung..
Attaches to underwater seal which provides negative
pressure and collects the drainage fluid.
The chest tube is placed in the 5th
ICS Anterior Axillary
Line within the triangle of safety. The triangle of safety
refers to the area within the mid-axillary line, anterior
axillary line, and 5th
ICS.
72.
Chest Tube
An alternativesite includes: the 2nd
ICS MCL (for
pneumothorax).
The chest tube is removed when it drains <1ml/kg/24hrs or
when it stops draining.
Thoracotomy is indicated for initial chest drainage of >1500 ml
or 3 consecutive hours of >200 ml per hour blood loss.
• Complications:
• Hemorrhage from intercostal vessel injury
• Subcutaneous emphysema
• Malpositioning into the lung parenchyma, liver, heart.
• Re-expansion pulmonary edema
• Obstruction from kinking, clots, tissue debris
• Dislodgement
• Infection
73.
Placement of ChestTube
• The patient is placed in a 30-60 degree reverse Trendelenburg
position
• The site is scrubbed with betadine/alcohol
• The site is anesthetized with lidocaine
• A 3-4 cm incision is made over the 5th
– 6th
rib b/w the mid-
axillary and anterior axillary line.
• Use a curved hemostat to puncture thru the intercostal
muscles and parietal pleura superior to the rib border.
• Perform finger exploration to confirm intrapleural placement
(feeling for diaphragm and intra-abdominal structures)
• Insert chest tube along side the finger
• Place the tube posteriorly and superiorly.
74.
Chest Tube
To calculatethe % pneumothorax, measure the
distance b/w the outline of the lung and the
chest wall. 1 cm = 10% up to 2.5 cm, then the %
increases.
It takes 300-500 ml of blood to blunt a
costophrenic angle.
If a central line is required, always place it on the same side as the
injury.
76.
Bronchoscope
•Flexible bronchoscope; passedthru nostril;
•Allows direct visual examination of the upper
airway and tracheobronchial tree, sampling of the
respiratory tract secretions and cell, and biopsy of
the airway, lung and mediastinal structures
•Uses: diagnostic and therapeutic
•Diagnostic: lung neoplasm and staging, assessment
of cough & wheeze of unknown origin, evaluation
of hemoptysis of unknown origin, identification of
etiologic agents in respiratory infections;
77.
Bronchoscopy
• Therapeutic: toremove retained secretions, pus, blood, or
foreign body from the tracheobronchial tree, to guide
insertion of a nasotracheal or orotracheal tube, and to instill
drugs directly to a specific lung area.
• Requirements: NPO for 4 hrs, Pre-medication with Atropine
and codeine, IV access, ECG and intermittent BP monitoring,
pulse oximetry, local anaesthesia, and sedation
• Complications:
• Respiratory depression from sedatives
• Hemorrhage (especially if biopsy is performed)
• Pneumothorax
• Cardiac arrhythmias
• Post bronchoscopy fever with no bacteremia
79.
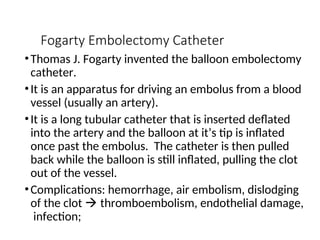
Fogarty Embolectomy Catheter
•ThomasJ. Fogarty invented the balloon embolectomy
catheter.
•It is an apparatus for driving an embolus from a blood
vessel (usually an artery).
•It is a long tubular catheter that is inserted deflated
into the artery and the balloon at it’s tip is inflated
once past the embolus. The catheter is then pulled
back while the balloon is still inflated, pulling the clot
out of the vessel.
•Complications: hemorrhage, air embolism, dislodging
of the clot thromboembolism, endothelial damage,
infection;
81.
Dacron Graft
•This isa 20 mm woven Dacron graft.
•It is a synthetic material used to replace or repair
blood vessels
•It is manufactured in either a woven or knitted
form. Woven grafts have smaller pores and do not
leak as much blood.
•Dacron grafts are frequently used in aortic and
aorto-iliac surgery. Eg. Aneurysm.
•Venous grafts have a superior result to synthetic
grafts when used below the inguinal ligament
82.
Dacron Graft
• Complications:
•Graft occlusion
• Graft infection
• True and false aneurysms at the site of anastomosis
• Distal embolisation
• Erosion into adjacent structures e.g. aorto-enteric fistulae
83.
Gortef/PTFE Graft
• PTFE(polytetrafluroethylene)/ Gortef is a synthetic vascular graft.
• Indications:
• As a vascular prosthesis for replacement or bypass of diseased vessels in
patients suffering occlusive or aneurysmal disease
• In trauma patients requiring vascular replacement
• For dialysis access or for other vascular procedures
84.
PTFE/ Gortef
• Contraindications:
•Should not be used as a patch leaking
• Should not be used for CABG or cerebral reconstruction procedures.
• Complications:
• Graft occlusion
• Graft infection
• True and false aneurysms at the site of anastomosis
• Distal embolisation
• Erosion into adjacent structures e.g. aorto-enteric fistulae
86.
Heparin
•Anticoagulant (inhibits formationof clots)
•Is used for DVT prophylaxis and Rx of DVT and
pulmonary embolism
•It bind to antithrombin III (a protease inhibitor) and
enhances (accelerates x1000) its activity (I.e. binding
to clotting factor protease enzymes inhibiting them
from activating the clotting factors).
•The prophylactic dose is 5000 U sc bid/tid
•It is contraindicated in persons who are
hypersensitive to the drug, are actively bleeding or
who have a bleeding dyscrasia, or post CNS surgery.
87.
Heparin
•Clexane is analternative to heparin
•It is low molecular weigh heparin
•It has smaller molecules and hence is less allergenic
than high molecular weight heparin
•It also has the advantage of less frequent dosing
(once daily).
•Other forms of DVT prophylaxis include:
• TED Stockings
• Early Stir up mechanism (early ambulation)
• Sequential Pneumatic Compression Stocking
88.
Heparin: DVT
• Patientsprone to developing DVT:
• Obese
• OCP use
• Long duration surgery
• Pelvic Surgery
• Hypovolemia and dehydration during surgery
• Malignancy (disseminated hematogenously)
• Hypercoagulable state
Hard Cervical Collar
•Used for all patients with a history of trauma,
especially if C-spine injury is suspected due to: injury
above the level of the clavicle, multiple injuries,
unconsciousness, neck pain, parasthesias, weakness,
paralysis or palpable deformity.
• The area most injured in the C-spine is C5-C6
because this area is most flexible but least stable.
• The disadvantage of the hard c-collar is that it is
uncomfortable for the patient, and allows for lateral
movement of the neck. It must therefore be used with
head blocks.
95.
C-spine Injury
• Afterinsuring that the airway, breathing and
circulation are secured, it is important to obtain a
lateral c-spine x-ray in order to determine whether or
not there is injury to the cervical spine.
• In the x-ray, one looks at 4 special lines:
o The anterior and posterior vertebral bodies
o The base of the transverse process
o The tip of the spinous process
• These 4 lines should all be straight. Subluxation of 3-
3.5 mm is abnormal. Assess for the thickness of the
soft tissue anterior to the body. This should not be
wider than the body itself.
96.
C-spine Injury
• Initialtreatment of C-spine fracture is by application of Gardner-
Wells Thongs/Calipers, and administration of steroids (solumedrol).
Solumedrol is given 30 mg/kg stat over 15 mins, then 5.4 mg/kg/hr
for 24 hours. The purpose for this is to decrease the swelling
which may lead to ischemia of the neurons above and below.
97.
Steroids
•High dose methylprednisolonesuccinate
(Solumedrol) is important in the management of
spinal injury
•Dose: 30mg/kg IV STAT over 15 mins followed
by: 5.4g/kg/hr IV over 24 hrs and up to 48 hrs.
•C-spine injury is most likely to occur at C5,C6 (the
most flexible portion)
•In assessing the patient, the anal tone is checked
(everything above S2-S5 is intact if normal); A
neurological examination should be done each time
the patient is moved.
98.
Steroids: Spinal Injury
•Repair:
•Spinal cord decompression laminectomy
• Steel rods
•Neurogenic Shock – a transient loss of tone
vasodilatation shock. NB There is hypotension*
and bradycardia (expected reflex is tachycardia). Rx:
administration of pressor agents
•Spinal Shock – a transient loss of reflexes and
flaccidity
•NB: Both conditions can coexist.
* One should not ascribe hypotension in trauma to neurogenic
shock. Hemorrhage should be suspected first.
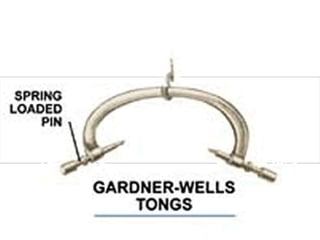
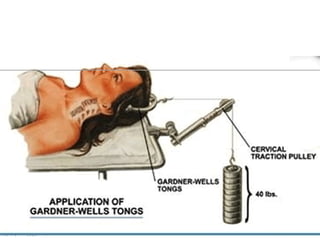
100.
Gardner Wells Tongs
•Thisdevice is used to provide cranio-cervical traction
•Indications:
• To reduce cervical spine fractures or dislocations
• To maintain alignment of reduced spine fractures
or dislocations.
• To immobilize the spine and prevent cord injury
• The Gardner-Wells tongs will usually be applied
by the Neurosurgeon in the ICU using local
anaesthetic, although light sedation may be
required. A spring loaded pin in one of the
handles will indicate the depth of penetration into
the skull.
101.
Gardner Wells Tongs
•Protrusion of the pin is 1.0 – 2.0mm into the skull
• The typical weight for simple cervical immobilisation is 10
lbs.
• Weight can be progressively added to reduce a
fracture/dislocation. The generally accepted maximum
weight is 140 lbs!
103.
Gardner Wells Tongs
•Twomajor complications with the use of
Gardner-Wells tongs:
• Penetration of the inner table of the skull by the
pins resulting in damage to the brain and
infection
• Loss of attachment by the pins and abrupt loss of
traction
•A 'hard' cervical collar of the correct size
should be kept at the bedside in the event
of traction failure
•Neurological status (motor and sensory
function) should be regularly checked while
a patient is in traction.
105.
20% Mannitol (Osmitrol)250 ml
• This is an osmotic diuretic
• It is used to reduce elevated ICP and IOP, to treat peripheral
edema, and to prevent and treat oliguria.
• Dose: 0.5-1 g/kg IV (50-100g) over 30-60 minutes 20g
in 100 ml = 50g in 250 ml
•Side Effects include:
• Hyponatremia and other electrolyte disturbances
• Pulmonary edema
• Metabolic acidosis
• Headache
• Dehydration
• Seizures
106.
Mannitol
• Other Methodsof Decreasing ICP:
• Elevation of bed head by 30 degrees
• Hyperventilation PaCO2 of 25-30 mmHg
• Shunt procedure to drain CSF (Ventricular)
• Craniotomy or Burr Hole
• Anaesthetic techniques: Lidocaine 100mg IV, Barbiturate coma (Thiopental 3-
5 mg/kg IV stat, then 1-2 mg/kg/hr
• Resection of mass lesion or silent parts of the brain (Rt. frontal lobe, anterior
temporal lobe)
107.
Phenytoin (Dilantin)
•Anticonvulsant
•It modulatesneuronal voltage-dependent sodium
and potassium channels (raises the seizure
threshold).
•It is given prophylactically for 48 hrs to persons with
depressed skull fracture
•Loading Dose: 750 mg over 30 mins
•Maintenance: 300mg/day
•Side effects: gingival hyperplasia, ataxia, nystagmus,
tremor; Hepatotoxicity, pancytopenia, arrhythmias.
Endotracheal Tube
• UncuffedEndotracheal Tube
Pediatric ETT
Size 2.0 (premature age)
Size 3.0 (newborns up to 2 yrs)
Uncuffed because the airways of a child are small, and provide
an adequate seal; A cuff can cause irritation edema
narrowing of the trachea respiratory embarrassment.
The tube is lubricated with sterile water because KY Jelly can
also edema and swelling.
Rx for broncho-oedema is racemic epinephrine (aerololized
epinephrine)
Because there is no cuff, a leak may be audible.
111.
ETT
Cuffed Endotracheal Tube
Internal diameter is in millimeters
Parts consist of the bulb, for inflation of the cuff; and a
universal adaptor for attachment to the breathing circuit.
Indications:
1. Any operation lasting >30 mins
2. Abdominal, thoracic & intracranial
procedures.
3. All surgeries of the head and neck.
4. All prone position surgeries.
112.
ETT
5. All fullstomach patients:
- Pregnant
- Emergency
- Intestinal Obstruction
- Diabetic
6. Unconscious patients (for airway protection)
7. Evidence of burns to the airway.
8. To provide positive pressure ventilation and PEEP.
9. To free the anesthetist’s hands.
113.
ETT
Signs of CorrectPlacement
1. Misting of the tube
2. Normal continuous wave form on the
capnogram.
3. Chest movements.
4. Bilateral breath sounds on auscultation.
Signs of incorrect placement of the ETT:
1. Tachycardia
2. Hypertension
3. Abdominal Distension
4. Desaturation
114.
ETT
Complications:
1. Sore throat(more in patients with irritable airways
eg. smokers, asthmatics)
2. Failed intubation (adequate oxygenation may be
maintained by face-mask).
3. Oesophageal intubation (must be recognized
rapidly, otherwise fatal)
4. Endobronchial intubation, recognized by:
Unequal chest movements
Lack of breath sounds on the left side of chest
Low blood oxygen saturations.
This is easily remedied by withdrawing the ETT a short
distance.
115.
Stylet
This is aninstrument used to facilitate proper
placement of the ETT
It is placed near the tip, but not past it, otherwise
perforation of trachea on insertion.
It ensures that the tip is rigid so that the tube can
be easily placed without wavering along its course.
Complications:
Perforation of the trachea hemorrhage
Perforation of the esophagus
116.
Laryngeal Mask Airway(LMA)
• It is a mask that fits over the larynx
• It is made of non-latex material
• It allows provision of positive pressure ventilation without visualization
of the vocal cords
• It does not protect the airway against regurgitation and pulmonary
aspiration
• It requires anesthesia for placement (topical, regional or general)
117.
LMA
•Indications:
• Surgeries lasting< 30 minutes in which an established
airway is needed
• Difficult intubation
• To guide ET tube placement
•It comes in 4 sizes (1-2 for Peds, 3-4 for Adults)
•It is inserted into the hypopharynx in its anatomical
position and then passed onward behind the larynx,
sealing the glottic opening, and enabling ventilation
after inflation of the cuff.
•A slight bulging of the tissues over the larynx
indicates the mask is properly positioned.
118.
LMA
• Complications:
• Laryngospasmin a lightly anesthetized airway
• Mal-placement
• Injury to surrounding structures
• Infection
• Aspiration
• Contraindications:
• Full stomach patients
• Procedures lasting >30 mins
• Allergy to the material
120.
McGill’s Forceps
Comes inAdult and Pediatric sizes.
It is used to aid the correct placement of the
nasotracheal tube.
The correct way to hold it is with the edges raised.
It grasps the tip of the tube, avoiding the cuff.
When one is doing a “blind” intubation and the
ETT is not going through, direct laryngoscopy
should be done to aid guiding the ETT into place
with the forceps.
122.
Nasogastric Tube (Ryle’sTube)
Closed active or passive drain
It has a radio-opaque line and 4 horizontal lines
Its uses are diagnostic and therapeutic
Diagnostic uses include: diagnosing the presence and
amount of blood in the stomach.
Therapeutic uses include:
1.decompression of the stomach
2.removal of activated charcoal given to children in
acute poisoning
3.nutritional (administration of enteral feeds)
4.administration of drugs
123.
NG Tube
Contraindications:
1.Basal skullfracture as evidenced by CSF otorrhea or
rhinorrhea, Battle’s sign (mastoid ecchymosis), or Raccoon
eyes (periorbital ecchymosis). CSF is confirmed by the ring
sign is by placing a drop of the bloody drainage on a piece
of filter paper, and looking for the Ring Sign. This is the
appearance of a yellow ring around the periphery of the
drop of blood.
2.Facial fractures.
The alternative to the nasogastric tube is the orogastric
tube which is placed orally using the McGill’s forceps.
Complication includes malplacement into the trachea
which may result in pulmonary aspiration and abscess.
125.
Chest Tube/ Tubethoracostomy
Closed active or passive drain
It is used for the drainage of blood, fluid, chyle or air from the
thoracic cavity, as well as for the restoration of negative pressure
in the thoracic cavity.
Attaches to underwater seal which provides negative pressure
and collects the drainage fluid
Advantages: permits the evacuation of blood, air, chyle, thus
expanding the lung
Disadvantages: can infect the thoracic cavity (empyema)
The chest tube is placed in the 5th
ICS Anterior Axillary Line within
the triangle of safety. The triangle of safety refers to the area
within the mid-axillary line, anterior axillary line, and 5th
ICS.
126.
Chest Tube/ Tubethoracostomy
An alternative site includes: the 2nd
ICS MCL (for
pneumothorax).
To calculate the % pneumothorax, measure the distance b/w
the outline of the lung and the chest wall. 1 cm = 10% up to
2.5 cm, then the % increases.
It takes 300-500 ml of blood to blunt a costophrenic angle.
If a central line is required, always place it on the same side
as the injury.
The chest tube is removed when it drains < 1ml/kg/24hrs or
when it stops draining.
Thoracotomy is indicated for initial chest drainage of >1500
ml or 3 consecutive hours of >200 ml per hour blood loss.
127.
Placement of TubeThoracostomy: Procedure
• The patient is placed in a 30-60 degree reverse Trendelenburg
position
• The site is scrubbed with betadine/alcohol
• The site is anesthetized with lidocaine.
• A 3-4 cm incision is made over the 5th
-6th
rib b/w the mid-axillary
and anterior axillary line.
• Use a curved hemostat to puncture thru the intercostals muscles
and parietal pleura superior to the rib border.
• Perform finger exploration to confirm intrapleural placement
(feeling for diaphragm and intrabdominal structures)
• Insert chest tube along side the finger
• Place the tube posteriorly and superiorly.
Central Venous Catheter
•A central venous catheter is used to gain access to a
central vein for:
• Monitoring of the central venous pressure
• Administration of drugs such as chemotherapy,
cardioactive drugs, and TPN.
• Indications: (Dignostic & Therapeutic)
• Measurement of central venous pressure (diagnostic)
• Administration of chemotherapy
• Administration of TPN (this requires a dedicated line)
• Hemodialysis
• Fluid administration when peripheral line are difficult (9 Fr)
• Long-term IV catheterization (i.e. >10 days)*
* Central lines at all sites should be changed every 3 days.
131.
Central Venous Catheter
Placement:Seldinger Technique (catheter over a guidewire):
1. First localize the vessel is using a small gauge needle.
Introduce a thin walled percutaneous entry needle into the
vessel.
2. Pass a guide wire through the needle; advance a portion
of the wire guide length into the vessel
3. Leaving the wire guide in place, advance the needle.
4. Enlarge the puncture site with a number 11 scalpel
blade
5. With a twisting motion, advance the catheter over the
wire guide and into the vessel.
6. After the catheter is in position, remove the guide wire.
The catheter is introduced into the Internal jugular, subclavian
vein, or femoral vein using an aseptic technique.
132.
Central Venous Catheter
GeneralComplications of Insertion:
Hematoma at the puncture site
Air embolism
Catheter tip embolism or loss of the guide wire
Hemothorax (except for femoral lines)
Diaphragmatic paralysis (from phrenic nerve injury) – except for
femoral lines
Arrhythmias (atrial or ventricular) –except for femoral lines
Complications Specific for Subclavian Puncture:
Brachial plexus injury
Internal mammary artery laceration
Pneumothorax
Subclavian artery puncture
Pulmonary emboli
133.
Central Venous Catheter
•Complications Specific to Internal Jugular:
• Carotid artery puncture hematoma, tracheal compression and
respiratory embarrassement; or dislodging of an atheromatous plaque
CVA
• Damage to the trachea or esophagus
• Complications of the Catheter Itself:
• Infection
• Thromboembolism
• Obstruction
• Displacement
• Complications of things put thru it:
• Hydrothorax
• Hydromediastinum
• Hydropericardium
• Obstruction
134.
Central Venous Catheter
OpenSurgical Exposure Technique
Requires an operating theater & general anesthesia.
Recommended for:
o Patients with respiratory disease
o Patients on a ventilator
o Patients with severe clotting disorders
Other forms of central venous catheters include:
Shiley Catheter for dialysis
Port-a-Cath for chemoRx
Perma-Cath for dialysis
Hickman Cath for dialysis
135.
Swan Ganz Catheter
•It is a pulmonary arterial catheter
• It is used for measurement of: Central venous pressure, Pulmonary
artery pressure, Pulmonary capillary wedge pressure, cardiac output,
pulmonary vascular resistance, and systemic vascular resistance.
• Its correct passage and placement by monitoring the changing
pressures as the tip moves from one region to another, and by
wedging of the catheter in the hilum (on CXR).
136.
Swan-Ganz Catheter
•Indications:
• Patientswith severe cardiopulmonary derangement (eg
HF, MI)
• Hypovolemic shock not responding readily to volume
replacement
• Sepsis with oliguria or hypotenstion
• Lung disorders at risk for associated myocardial dysfn.
• Failure of 2 or more organs
• Procedures in which large volumes are required or large
fluid shifts eg abdominal aortic surgery
137.
Swan-Ganz Catheter
• Complications:
•Same as for central venous catheter
• Complications unique to Swan-Ganz:
• Ventricular arrhythmias
• Ventricular rupture
• Valvular damage on the right side of the heart
• Intra-cardiac knotting of catheter
• Pulmonary infarction induced by permanent wedging of the catheter in the distal
pulmonary vascularture
• Perforation of the pulmonary artery (rare)
139.
Urinary Catheter
Double lumenurinary catheter
Is a closed, passive drain
It has 2 lumens, one for drainage and the other for
inflation of the bulb which anchor the catheter in the
bladder, hence making it self-retaining.
Uses:
1. To decompress the urinary bladder, e.g. Acute
urinary retention. (a Coude cath is used if this fails)
2. To monitor urinary output intra-op, or in patients in
shock.
3. To divert the urine stream in patients who have had
an incision & drainage of an abscess of the
perineum.
140.
Urinary Catheter
Contraindications:
Traumato the urethra as evidenced by blood
in the meatus.
Pelvic fracture
A high riding prostate, or boggy mass below
the prostate upon digital rectal examination.
Urethral tears can be investigated by placing
the foley catheter partly in the urethra and
instilling 50cc of Urograffin dye as a pelvic x-ray
is shot. A retrograde cystourethrogram is
created. If there is rupture, then dye will be seen
leaking into the surrounding tissues.
142.
Laryngoscope & Blade
Preventionof the HTN Response to Laryngoscopy:
Give deep anesthesia
Give 50-100 mcg of fentanyl 2 minutes prior to
laryngoscopy
Give 50-100 mg of lidocaine 2 minutes prior to
laryngoscopy
Give a small dose of a short acting beta blocker eg.
Esmolol 5-10 mg, immediately before intubation
(Avoid in irritable airways)
145.
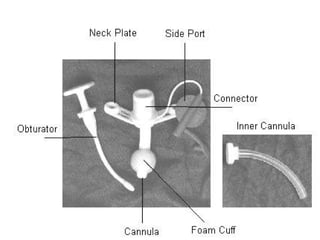
Tracheostomy tube
Plastic CuffedTracheostomy Tube
Cannula - can be outer and inner
Obturator is used to clear anything that obstructs
the tube.
1. Eg. crusted blood
2. Mucous plug
3. Secretions
Inflatable cuff - enough air put into prevent a leak.
Flange - for suturing to skin.
Strap/Tape - to secure around neck
146.
Tracheostomy
Indications:
1. Prolonged intubation> 2/52
2. Respiratory Toilet (easier suctioning with
tracheostomy than ETT)
3. Trauma to facial bones
4. During failed oro/naso-tracheal intubation.
5. Prophylactically in ENT surgery or head surgery.
6. Upper airway obstruction (esp mechanical
obstruction, because oedema can be treated with
epinephrine before doing a tracheostomy.)
Care of TracheostomyTube:
Dressing - change every 2 hrs or more frequently if it
becomes saturated. (NB moist dressings act as a
breeding ground for bacteria)
Note the type of drainage from drainage from
tracheostomy
Incision site must be inspected and cleaned with
hydrogen peroxide and sterile water with each dressing
change.
Nitrofurazone ointment is applied if there is any sign of
local infection.
If the tracheostomy tube has an inner & outer cannula,
the inner cannula should be removed every 2-4 hrs for
the first 24 hrs, cleaned with a tracheostomy brush,
hydrogen peroxide, and sterile water.
149.
Care of Tracheostomy
NBAlways keep a spare tracheostomy tube handy in
case the need for it arises.
Frequent suctioning (Based on volume & character of
patient’s secretions). Suctioning orders should be written
as prn orders. Some patients need constant suctioning
initially; eg. Fulminant pulmonary edema. However,
unnecessary suctioning may lead to undue irritation of the
tracheobronchial mucosa and actually cause extensive
production of mucus.
Tracheostomy tubes should be changed on a regular
basis (eg. q7 days). This allows for total inspection of the
tracheal stoma and the tube itself.
151.
Intraosseous Infusion Needle
•Inchildren, an intraosseous infusion needle may
be sued to instill fluid into the bone marrow cavity.
The site selected is 2-3 cm below the tibial
tuberosity. The tibia is used because its plate has
not closed as yet. The intraosseous infusion needle
is driven into the bone marrow cavity in a screwing
motion. Bone marrow is aspirated back, and 10cc
of saline is instilled. If this flows easily, then the IV
fluid is connected.
152.
Intraosseous Infusion Needle
Complicationsof intraosseous infusions:
•Osteomyelitis
•Cellulitis
•Damage to the epiphyseal plate if placed in the
wrong location.
•Injury to muscle
•Injury to nerves.
154.
Oropharyngeal (Guedel) Airway
•Itis a device that is placed into the oral cavity to
prevent the tongue from falling back and obstructing
the airway
•It is used in persons who don’t have a gag reflex
•It is inserted with the tip pointed up, and then
rotated 180 degrees pushing the tongue to the side
•It has a port for allowing suctioning
•Complications:
• Can precipitate vomiting in persons with a gag reflex
• May cause cervical movement spinal damage in a
person with c-spine trauma
• Can cause elevation of ICP.
• Injury to oral mucosa or teeth
155.
Nasopharyngeal Airway
• Alsocalled the “trumpet”
• It is a flexible, soft rubber airway which is placed in the more patent
nostril.
• It can be used without anesthesia
• It is better tolerated than the oropharyngeal airway
• Complications:
• epistaxis
Plaster of Paris/Gypsona
•This is anyhdrous calcium sulphate
• It is rehydrated in water and applied over under-cast padding to
form a hard cast.
• It’s disadvantages include:
• Heavy weight (compared to fiberglass)
• Itching that is not easily accessible
• Requirement that the cast remains dry
161.
Intramedullary Nail
Thisdevice is used as a means of internal fixation
It is suitable for fractures of the long bones
especially when the fracture is near the middle of the
shaft
Bones repaired include:
o Femur
o Tibia
o Humerus
o Ulna??
It has transverse perforations at regular intervals
only at the ends to allow the insertion of transfixation
(locking) screws through bone and thus afford rigidity
and resistance to rotation forces.
162.
Intramedullary Nail
The rodis inserted into the tibia by splitting the
patella tendon fibers and drilling a hole thru the tibial
plate, and reaming the rod thru the tibial marrow
cavity.
The site of insertion for fixation of femoral shaft
fractures is the piriform fossa.
Advantages:
o ORIF can be done under direct visualization
o The patient can be mobilized sooner.
Contraindications:
o Osteomyelitis
163.
Acute Specific Complications:
Hemorrhage
Infection (4-5th
day)
Neurovascular injury
DVT -80% proximal
Failure of fixation
1. Nail too long or too short
2. Nail jammed in femur
3. Failure to get locking screw thru hole in nail
# of neck or shaft of femur when placing nail
Guide wire driven into knee
164.
Longterm Specific Complications
•Failureof fixation (loosening and migration)
•Malunion or Nonunion
•Osteonecrosis
•Osteomyelitis
•Heterotopic ossification
•Post-traumatic arthritis
•Reflex sympathetic dystrophy
166.
Richard Dynamic CompressionHip Screw
It is indicated for treatment of
intra-trochanteric/pertrochanteric fractures
The Richard Classic is specifically indicated for
subtrochanteric fractures.
It is made up of two parts which can slide in relation
to each other but do not allow binding.
The 1st
part is a heavy-duty plate which is fixed to the
lateral cortex of the femur with cortical screws.
The 2nd
part is a rod, which passes up through a slot in
the plate into the femoral neck. Its threaded end
crosses the fracture line to engage and hold the
femoral head.
167.
Richard Dynamic CompressionHip Screw
As the patient weight-bears on the healing fracture the broken ends
of the bone collapse into each other and compress the fracture.
The sliding-rod mechanism of the dynamic hip screw allows this to
happen without allowing the hip to fall into varus. This prevents the
plate breaking at the fracture, or the rod penetrating through into the
femoral head and aceabulum
Skin Traction
• Skintraction can only be done up to
7 lbs or 1/7 – 1/10 body weight.
172.
Skeletal Traction
• Skeletaltraction is 1/5 to 1/7 of total body weight.
• The knee (high tibial) takes up to 30 lbs.
• The adequacy of skeletal traction is assessed in 48
hours by comparing the lengths of the femurs (from
ASIS to tibial tuberosity).
• Sites for Skeletal Traction:
• Greater trochanter (for central dislocation of hip)
• Lower femoral (for femoral #, however may get in the
way of an intramedullary pin)
• High Tibial [most common] – (for femur fractures)
• Lower Tibial (for tibial fractures)
• Calcaneum (for some calcaneus fractures)
174.
Austin Moor Hemi-Arthroplasty
Artificialhip replacement
Indications:
Elderly persons who fall and fracture their hip
(Garden Class 3 & 4 fractures of the neck of the femur)
Osteoarthritis
Avascular necrosis of the head of the femur eg. sickle cell disease
Watson Modified HumbyKnife
•The humby knife is manually powered and has
adjustable rollers that control the thickness of the graft.
•It can be used to harvest long narrow grafts of split
thickness skin from the thigh, arm or abdomen.
•Once the graft has been harvested the tissue is laid atop
the wound and is secured using methods that include
skin suture, staples or tape. All areas of the wound
should be covered by the grafted skin with adequate
fenestrations to allow for fluid escape from beneath the
grafted skin.
184.
Skin Grafts
• Whatmust you ensure before taking a skin graft?
1.The donor site must be free of infection.
2.There must be good vascularity.
3.There must be no necrotic tissue present
• Indications for a skin graft:
1.Burns involving the epidermal appendages (which are
necessary for proper wound healing).
2.Large partial thickness burns.
3.Replacement of skin surgically removed because of
melanoma, or other purpose.
4.Skin Ulcers.
185.
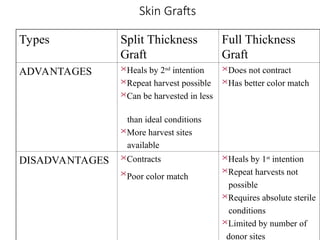
Skin Grafts
Types SplitThickness
Graft
Full Thickness
Graft
ADVANTAGES Heals by 2nd
intention
Repeat harvest possible
Can be harvested in less
than ideal conditions
More harvest sites
available
Does not contract
Has better color match
DISADVANTAGES Contracts
Poor color match
Heals by 1st
intention
Repeat harvests not
possible
Requires absolute sterile
conditions
Limited by number of
donor sites
186.
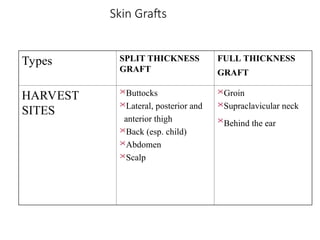
Skin Grafts
Types SPLITTHICKNESS
GRAFT
FULL THICKNESS
GRAFT
HARVEST
SITES
Buttocks
Lateral, posterior and
anterior thigh
Back (esp. child)
Abdomen
Scalp
Groin
Supraclavicular neck
Behind the ear
188.
1% Silver Sulphadiazine
•Is a topical anti-microbial agent used in the treatment
of burns.
• INDICATIONS:
Silver sulphadiazine is a topical antibacterial agent for
the prevention of infection in severe burns being
particularly effective against Gram-negative organisms
such as Pseudomonas aeruginosa and pyocyanea, the
most common cause of burn wound infection.
• Advantages:
(i) inexpensive
(ii) painless to apply
(iii) does not stain tissues
(iv) has broad spectrum activity
189.
1% Silver Sulphadiazine
(v)The slow liberation of silver does not cause the rapid and
extensive depletion of chloride ion experienced when silver nitrate
solutions are used, and thus electrolyte disturbances are minimised.
• Disadvantages:
(i) Cannot be used in persons allergic to sulfur
(ii) Does not penetrate escar
(iii) Does not penetrate cartilage
(iv) A 3-5 mm thick layer is needed
(v) Separation of the eschar may be
delayed.
(vi) Local skin sensitivity may occur especially
when exposed to sunlight.
190.
Silver Nitrate
•It isa topical anti-microbial agent used in the
treatment of burns.
•Disadvantages:
•(i) It stains the tissues black and slows healing
•(ii) It is painful to apply
•(iii) It bleaches chloride from the skin, thus can
• cause hypochlorosis
•(iv) Is in liquid for that requires supervision for
• q2h soaks (time consuming)
191.
Malfinide Acetate 0.5%
•It is a topical antimicrobial agent used in the treatment of burns.
• Advantages:
(i) penetrates escar well
(ii) penetrates cartilage well (thus can be
used on ears and nose)
• Disadvantages:
• (i) It inhibits bicarbonate production acidosis
• (ii) It is not easily available
193.
Fluid Resuscitation (Day1)
• Parkland Formula:
• Wt (kg) x %TBSA Burns x 4 = Total fluid for 24 hrs. (Use Lactated Ringers because
it is physiologically the closest to plasma).
• 1st
½ is given within 8 hrs from the time of the burn.
• 2nd
half is given over the remaining 16 hrs.
• Replace any ongoing losses eg. Urine, oozing from the wound, etc.
• Urine output must be maintained at > 0.5 – 1 ml/kg/hr
195.
Fluid Resuscitation (Day2)
• Add a colloid solution at 0.3 - 0.5ml / kg / TBSA Burns
• Colloids are not used on Day 1 because of the acute inflammation
that is ongoing which results in widening of the vascular pores
increased leakiness loss of proteins. By day 2 the pores are not as
leaky.
196.
Fluids
• Crystalloids arefluid substances which are able to
cross a semi-permeable membrane. It is usually
composed of at least one solute and water. They are
used for fluid and electrolyte resuscitation in trauma or
shocked patient, burns, dehydration secondary to
diarrhea/vomiting/ or reduced intake, for maintenance
fluids in patients who being kept NPO, as a medium to
give drugs which must be diluted.
• In hemorrhagic shock, for each mL of blood loss, 3-5
mL of crystalloid is given for replacement. If the patient
is elderly or has cardiac disease, then replacement is
3ml per 1mL of blood loss. 30-40% of the crystalloid
infusion stays in the intravascular space.
197.
Fluids
• Examples ofcrystalloids include:
• 0.9% NaCl 1 Liter bag.
• 5% Dextrose in Water
• Ringers Lactate
• D5E48
•Complications of administration of crystalloids
include:
• Volume overload
• Shock from administration of cold fluid
• DIC secondary to dilution of clotting factors
• Electrolyte disturbances
198.
Colloids:
• Colloids arefluid substances which are used for
fluid replacement therapy. They are used
especially in patients who are hypotensive or are
hypovolemic. They do not cross semi-permeable
membranes easily because their molecules are
large. Colloid are given after 2-3 L of crystallid is
given, in order to avoid the complications of giving
too much fluid.
• Example of colloids include:
• Hexastarch (6% Hexose)
• Dextran
• Albumin
• Blood
199.
Colloids
Complications include:
Allergic reactionswith Dextran
Hexastarch interferes with cross-matching of blood
Introduction of infection
Thrombophlebitis
The first choice of blood used in trauma is O-negative.
The next choice of blood used in trauma is type-specific.
But the best choice of blood to be used is cross-
matched blood.
200.
Colloids
Complications of bloodtransfusion:
• Hemolytic transfusion reaction
• Infections such as Hep B & C, HIV, CMV
• Iron Overload (250 g of iron per unit)
The Urethra
• Consistsof:
• Bulbous Urethra
• Penile Urethra
• Membranous Urethra
• Prostatic Urethra
• The diameter is 22-24 F
• Commonest reason for
205.
Urethral Dilator/Sound
The shortstraight one is for females
The long curved end one is for males (it is curved so
that it can get over an enlarged prostatic middle
lobe)
It is used in patients with urethral strictures such as
those with prior instrumentation or gonococcal
urethritis.
The stricture is “dilated up” gradually (over several
weeks)
There are two numbers (one represents the tip and
the other the shaft diameter)
206.
Urethral Dilator/Sound
Complications:
Creation of a false passage (rupture of urethra)
Hemorrhage
Common Sites of Stricture formation:
1. Bulbous urethra
2. Peno-scrotal junction
3. Membranous urethra
Stricture rarely occur in females, and when the do
occur, they occur in elderly females at the external
uretheral meatus.
208.
Jake’s Urinary Catheter
Closed,passive drain; It is non-self retaining
Used to decompress the urinary bladder during
laparoscopic surgery prior to insertion of the
umbilical port (hence reducing the likelihood of
complications); or to obtain a clean catch specimen
(eg. in a patient who is menstruating); or to empty
the urinary bladder prior to delivery of the fetus
It is less expensive than a Foley’s catheter
It is made of red rubber which can cause severe
tissue reaction if left in place for long periods of time.
(complication)
209.
Double Lumen FoleyCatheter
Is a closed, passive drain; It is self retaining
It has 2 lumens, one for drainage and the other for
inflation of the bulb which anchor the catheter in the
bladder, hence making it self-retaining.
Uses:
1. To decompress the urinary bladder, e.g. Acute
urinary retention.
2. To monitor urinary output intra-op, or in patients in
shock.
3. To divert the urine stream in patients who have
had an incision & drainage of an abscess of the
perineum.
210.
Double Lumen FoleyCatheter
Contraindications:
Trauma to the urethra as evidenced by blood in
the meatus.
Pelvic fracture
A high riding prostate, or boggy mass below
the prostate upon digital rectal examination.
•Urethral tears can be investigated by placing the
folley catheter partly in the urethra and instilling
50cc of Urograffin dye as a pelvic x-ray is shot. A
retrograde cystourethrogram is created. If there is
rupture, then dye will be seen leaking into the
surrounding tissues.
211.
Triple Lumen FoleyCatheter
This is a 24 french triple lumen foley catheter (24 F is
the external diameter).
It is closed passive drain; It is self retaining
Has a lumen for inflation of the balloon, one for
drainage of the bladder, and the 3rd
for introduction of
medication, and introduction of sterile crystalloids
(used for irrigation of the bladder.
Used in:
Patients requiring long-term catheterization
Patients undergoing TURP or an other procedure in which
significant hemorrhage is expected (a 30cc balloon is
required for TURP surgery)
Patients with massive hematuria
212.
Triple Lumen UrinaryCatheter
•Complications of Placement:
• Inadequate lubrication of catheter friction trauma
hemorrhage, and eventually stricture formation after
healing.
• Use of an introducer during placement can false passage
• If the balloon is inflated while in the urethra, this can
rupture of the urethra and hemorrhage.
•Complications of the Catheter insitu:
• Infection
• Dislodgement
• Obstruction
• Stone Formation
213.
Triple Lumen FoleyCatheter
• Complications of things put thru the Catheter:
• TURP Syndrome – Instillation of hypotonic fluids for too long a duration
hyponatremia seizures
• A triple Lumen Urinary catheter can be kept insitu for a maximum of 3
months before requiring replacement.
215.
Cystoscope
•A thin, lighted(usually fiber optic) instrument
used to look inside the bladder and remove
tissue samples (biopsy) or small tumors.
•The indications for cystoscopy include:
• The evaluation of blood in the urine (hematuria),
• Evaluation for strictures
• Removal of stents,
• Various other reasons, including evaluation of
prostate anatomy before consideration of prostate
surgery.
216.
Cystoscopy: Procedure
• Theflexible cystoscope is connected to water irrigant, and a light source.
Inside the urethra and bladder are viewed thru a lens. The urethra is first
entered and inspected, and then the bladder is entered. The doctor will
survey all areas of the bladder and inspect the urine coming out of the
ureteral openings.
217.
Cystoscopy: Complications
•Hematuria fora few days or even up to a week or
so, and may have a slight bloody urethral
discharge. This is all normal and should improve.
•Urethral spasms, or a frequent/urgent need to
void. All this is normal and should also go away
soon.
•Serious infections or other complications are
exceedingly rare after office cystoscopy.
218.
Pigtail Ureteral Catheter
Closedpassive drain
Used in percutaneous nephrostomy for drainage if the kidney
Complications:
Stone formation with prolonged placement
Infection
Obstruction
Displacement
220.
Double J StentCatheter
Is a closed passive drain
It is self retaining
Has a kidney end (that passes into the renal pelvis) and a bladder
end
It is used to bypass obstruction or after ureteric surgery to stent
the ureter.
To decompress the kidney to relieve obstruction of the ureter
(usually by calculus)
221.
Non Self-Retaining UreteralCatheter
Is a non-self-retaining ureteral catheter / stent
Is used for:
exploring the ureter
anterograde pyelography
checking for reflux of urine
• Is placed via a cystoscope
223.
Urograffin Radiocontrast Dye
•UrograffinRadio-Contrast Dye
Intravenous, Water soluble contrast dye
Used to show the anatomy and function of the
kidneys (IVP shows anatomy and function, Retrograde
Cysto-urethrogram demonstrates anatomy only)
Patients normally experience a metallic taste in the
mouth
Complications:
Allergic reaction if allergic to shell fish
224.
Urograffin Radiocontrast Dye
Patientshaving an allergic reaction may appear
diaphoretic, short of breath, have wheezing, urticaria.
Treatment of the allergic reaction:
1.Stop infusing the contrast
2.Give fluids
3.Administer antihistamines (eg Piriton)
4.Give glucocorticoids (eg. hydrocortisone)
5.If necessary, give subcutaneous epinephrine.
•Contrast induced nephropathy renal failure (hence
BUN, Creatinine and Electrolytes should be done prior
to administration of dye)
225.
Urograffin Dye
• Inpatients known to have a minor reaction to the dye (eg. Urticaria),
antihistamines may be given prior.
• Alternatively, the patient can be given Ultra-vist which contains low
molecular weight iodine which is less allergenic.
227.
Self-Retaining Suprapubic Catheter
•Suprapubic Cystostomy (procedure)
• Direct puncture of the bladder through the abdominal wall
with introduction of a catheter over the needle and guide wire
is the method used. Anticholinergics are given to reduce
bladder spasticity.
• Indications:
• Failure of clean intermittent catheterization
• Irrigation of the bladder if no 3-way catheters are available
• Advantages:
• significantly lower incidences of urinary tract infections than chronic
indwelling urethral catheters and even intermittent catheterization.
Total Parenteral Nutrition
•Nephro, Criticare HN, & Glucerna Nutritional Supplements
• TPN is a complete form of nutrition, containing protien,
sugar, fat, and added vitamins and minerals as needed for
each individual. It is admininstered through an intavenous
infusion, usually using a central line. A central line is a
special long lasting IV line that goes through a vein directly
to the heart.
235.
Surgical Stapeler
Stainless steelstaples used for approximation of skin (eg. Abdominal
wall or neck eg post thyroidectomy), and bowel anastomosis.
Has the advantages of rapid and technically easier tissue approximation,
better cosmetic results, minimal allergic and tissue reactions
Disadvantage – higher cost.
237.
Nylon Suture
Synthetic
Non-absorbable
Monofilament
Used forskin closure, plastic surgery, neurosurgery, ophthalmology,
retention, microsurgery (eg. vascular grafts), abdominal fascia and linea
alba.
Has poor memory, therefore several knots must be made for the suture
to hold.







































![Skeletal Traction
• Skeletal traction is 1/5 to 1/7 of total body weight.
• The knee (high tibial) takes up to 30 lbs.
• The adequacy of skeletal traction is assessed in 48
hours by comparing the lengths of the femurs (from
ASIS to tibial tuberosity).
• Sites for Skeletal Traction:
• Greater trochanter (for central dislocation of hip)
• Lower femoral (for femoral #, however may get in the
way of an intramedullary pin)
• High Tibial [most common] – (for femur fractures)
• Lower Tibial (for tibial fractures)
• Calcaneum (for some calcaneus fractures)](https://image.slidesharecdn.com/surgeryinstruments-250323065120-665859d8/85/Surgery-Instruments-presentation-for-medical-students-172-320.jpg)