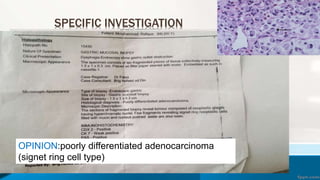
This document presents two case studies of patients with gastric cancer. The first case is a 60-year-old male who presented with epigastric pain and vomiting for two months. Various tests were performed and it was determined that he had a signet ring cell type adenocarcinoma of the stomach. He underwent a laparoscopic gastrectomy. The second case is a 72-year-old male who also presented with epigastric pain and chest heaviness. He was found to have adenocarcinoma of the stomach as well and underwent a laparoscopic gastrectomy. The document then provides further details on the anatomy, histopathology, classification, staging, signs and symptoms, and management of







































































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
