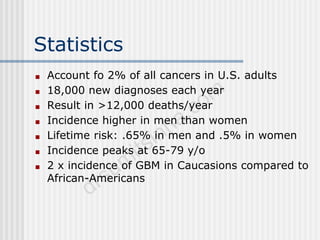
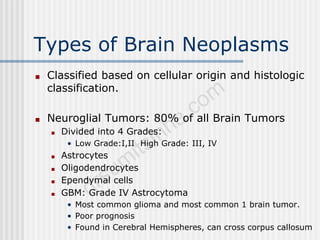
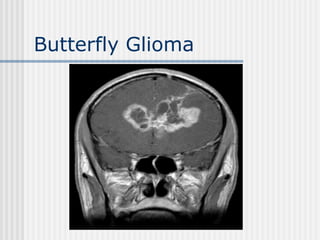
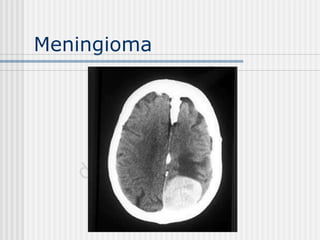
Primary CNS tumors account for 2% of cancers in adults in the US, with over 18,000 new cases diagnosed each year resulting in more than 12,000 deaths. The most common type is glioblastoma, which has a poor prognosis. Risk factors include high dose radiation exposure and certain genetic syndromes. Symptoms vary based on location but often include headaches, cognitive changes, and seizures. Diagnosis involves imaging, typically MRI with contrast, followed by histopathology. Treatment options include surgery, radiation therapy, and chemotherapy, with the standard of care for high grade gliomas being radiation plus temozolomide.