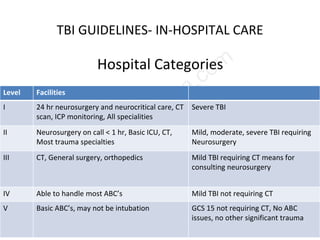
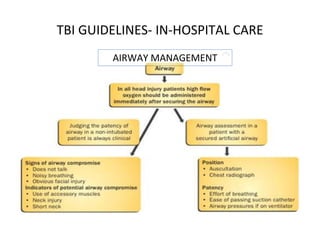
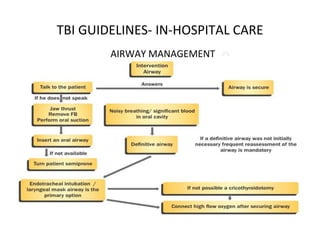
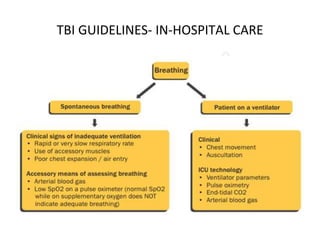
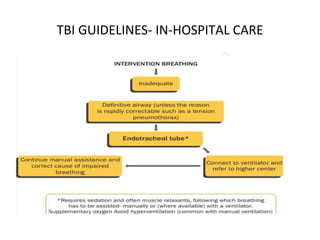
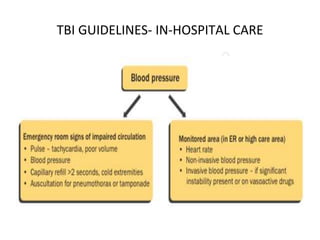
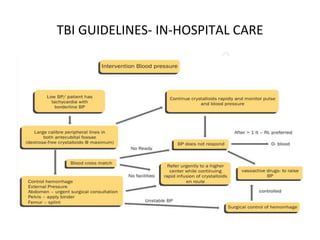
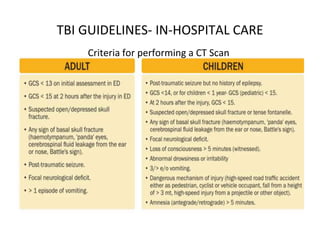
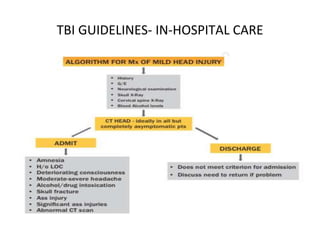
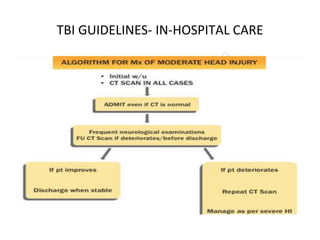
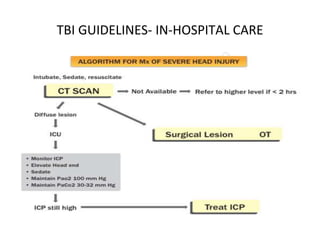
This document outlines guidelines for in-hospital care of traumatic brain injury (TBI) patients in India. It notes that trauma care systems are nascent and there is a lack of organized protocols. Guidelines are needed to standardize prehospital and hospital critical care as available personnel and skills often do not match patient needs. The document then proposes a 5-level categorization of facilities based on available services and recommends minimum standards. It provides guidance on airway management, clinical monitoring, indications for admission and CT scanning, and in-hospital management considerations like nutrition, DVT prophylaxis, and discharge/follow-up. The conclusion states that while formulation of guidelines may not be difficult, enforcement will be a challenge that requires collective effort