Downloaded 19 times



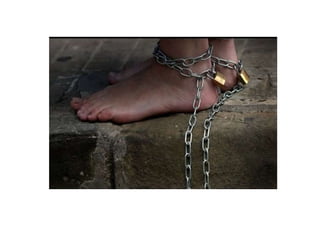


This document discusses various topics related to forensic psychiatry including: 1. Types of delusions such as delusions of persecution, grandeur, and infidelity. 2. Types of hallucinations including visual, auditory, olfactory, tactile, and psychomotor hallucinations. 3. Legal tests for insanity such as the M'Naghten rule, which states that to use insanity as a criminal defense, the accused must not have known the nature or quality of their actions, or that they were wrong, due to mental illness. 4. Responsibility and restraint considerations for the mentally ill, including admission criteria and limitations on certain treatments without proper approval.











































![Mental health legislation altaf qadir [autosaved] usman ppt](https://cdn.slidesharecdn.com/ss_thumbnails/mentalhealthlegislationaltafqadirautosavedusmanppt-200323165733-thumbnail.jpg?width=640&height=640&fit=bounds)











































