This document provides information on forensic psychiatry and aspects related to determining criminal responsibility for mentally ill individuals. It discusses key topics such as:
- Forensic psychiatry deals with applying psychiatric knowledge to legal and justice systems.
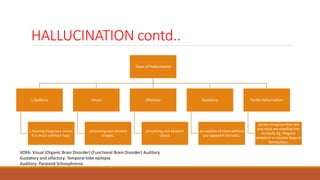
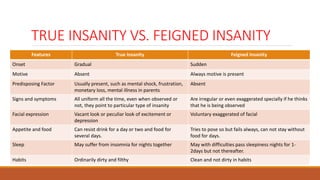
- Various mental states and disorders are described, including hallucinations, delusions, and impulse control issues.
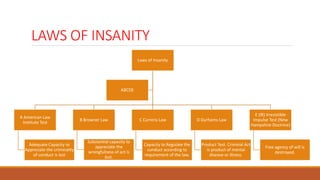
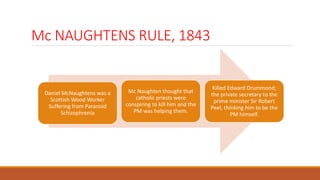
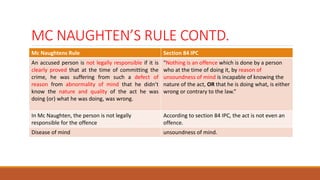
- Laws and tests for insanity are outlined, including McNaugthen's Rule which established the insanity defense.
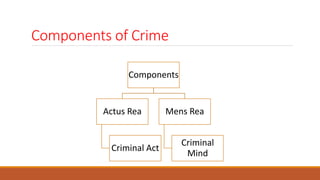
- Civil responsibilities and ability to enter contracts are impacted by mental illness. Criminal responsibility depends on understanding the nature and wrongfulness of one's actions.