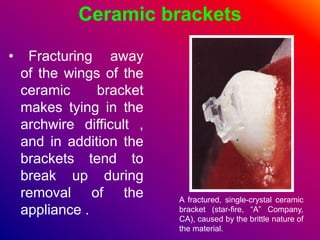
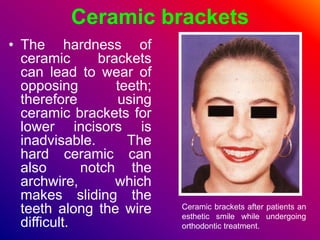
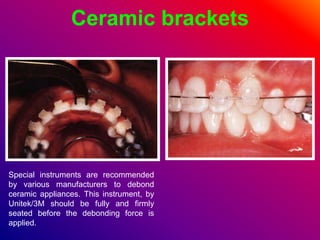
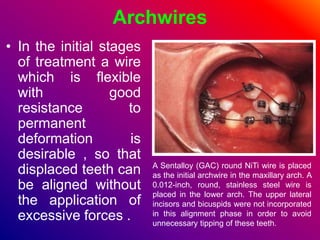
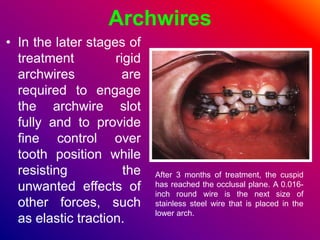
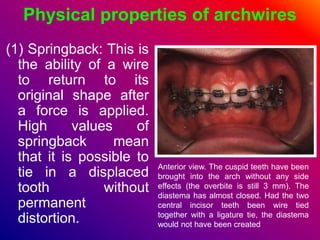
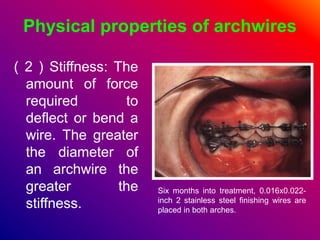
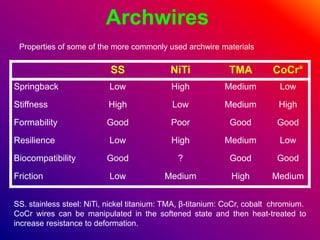
This document discusses ceramic brackets and archwires used in fixed orthodontic treatment. It notes that ceramic brackets can fracture and be difficult to remove. It also states that the hardness of ceramic brackets can cause wear on opposing teeth. The document discusses different types of archwires used at various stages of treatment, including more flexible wires initially to align teeth and stiffer wires later for more precise control. It also summarizes properties of archwires like springback, stiffness, formability and resilience.






































































![Recent Advances in Archwires [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/recentadvancesinarchwiresautosaved-250607082542-51523f1a-thumbnail.jpg?width=640&height=640&fit=bounds)


![100013603 [Repaired] [Auto-saved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/100013603repairedauto-saved-240104174437-00157480-thumbnail.jpg?width=640&height=640&fit=bounds)








































