Downloaded 232 times



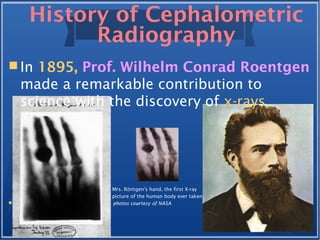
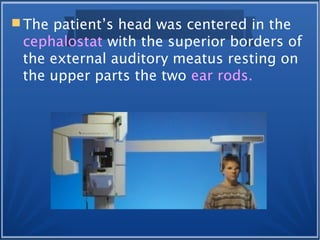



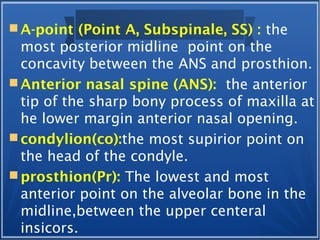




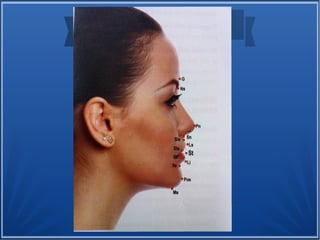


This document provides a history of cephalometrics and landmarks used in cephalometric analysis. It begins with early attempts to classify human physiques prior to radiography. In the late 19th century, x-rays were discovered, allowing for visualization of cranial structures. In the 1920s, standardized lateral cephalograms were developed, and cephalometric analyses were created to quantify skeletal and dental relationships. The document outlines the contributions of key figures and describes commonly used cephalometric landmarks on hard and soft tissues.





















































![ceph_LLP_SEMINAR[2].pptx landmarks lines and planes](https://cdn.slidesharecdn.com/ss_thumbnails/cephllpseminar2-250919182304-905904ac-thumbnail.jpg?width=640&height=640&fit=bounds)



































