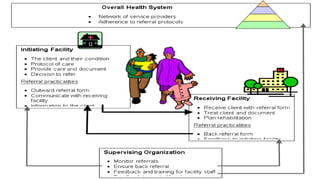
This document discusses the referral health mechanism in Nepal. It begins by defining referral as the process where a health worker seeks assistance from a better resourced facility to manage a client's condition. Key reasons for referral include seeking expert opinion, additional services, admission, or diagnostic/therapeutic tools.
The characteristics of an effective referral system are described as ensuring close relationships between health levels to provide the best possible care closest to home, making cost-effective use of services, and building capacity through support between levels.
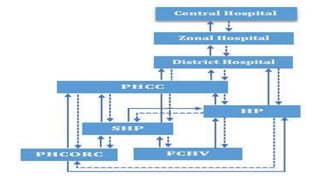
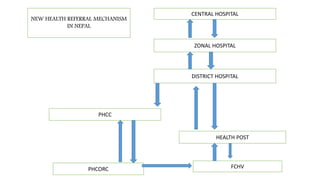
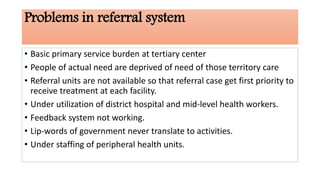
The current referral hierarchy in Nepal is outlined, with health posts as the first contact point referring to primary health centers and up to district, regional and specialty centers. Problems include inappropriate use of tertiary facilities and