
Download as PPS, PPTX




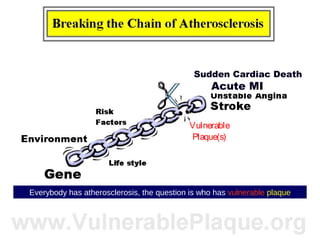
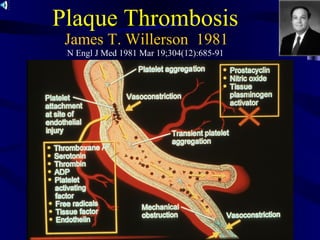
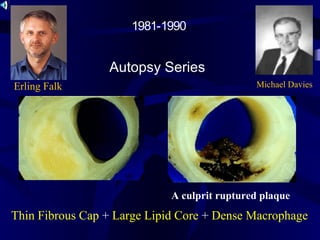
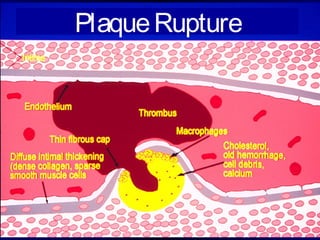
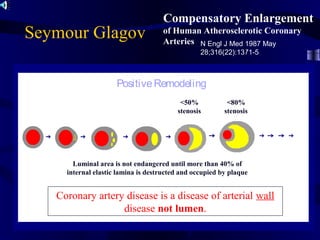
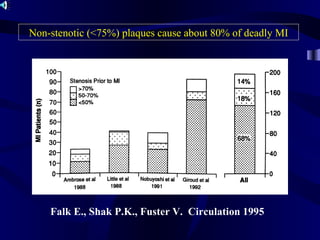
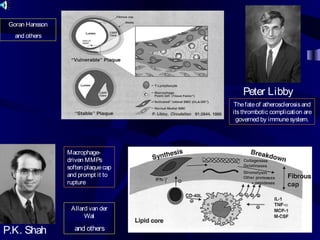
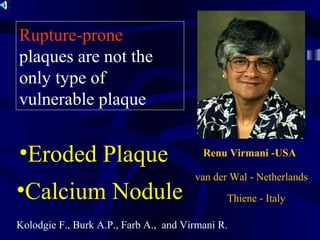
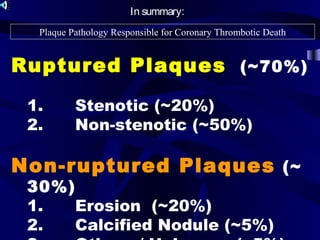
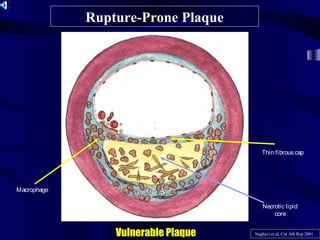
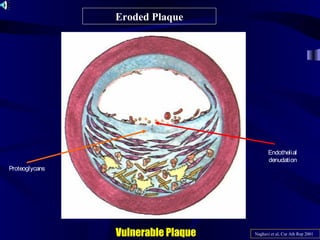
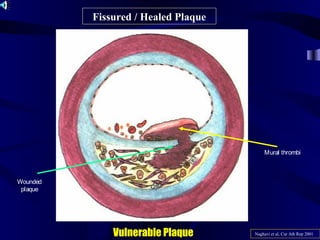
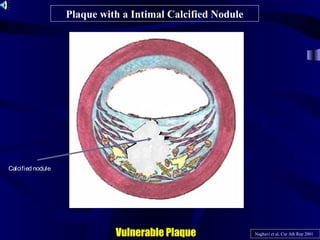
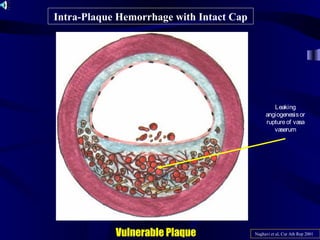
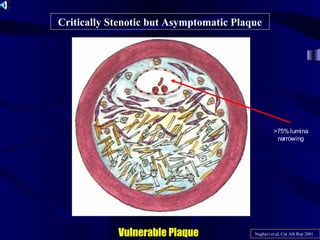
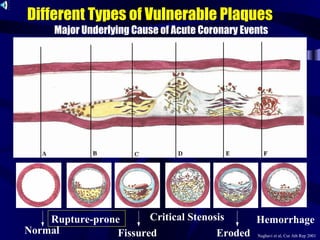
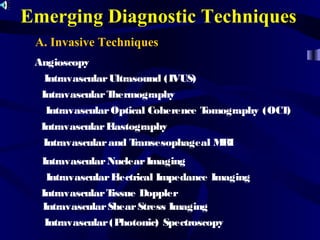
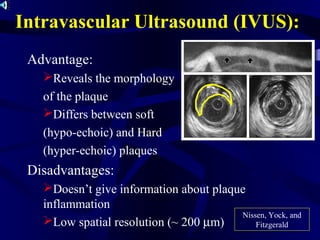
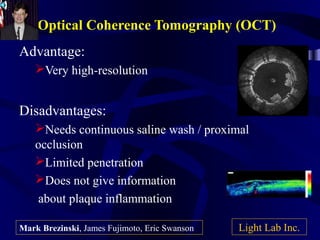
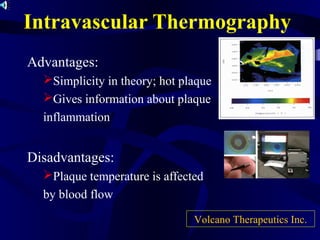
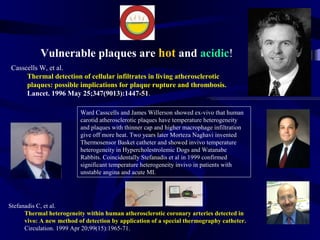
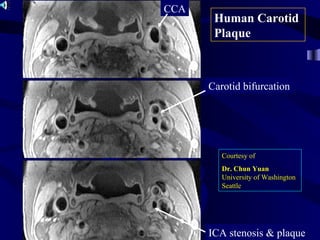
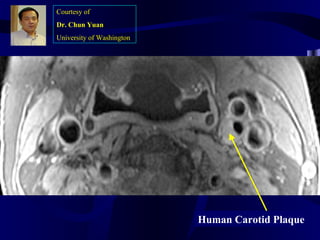
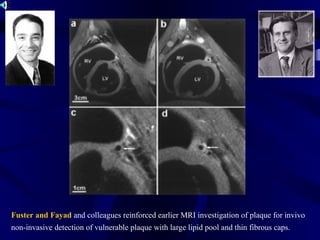
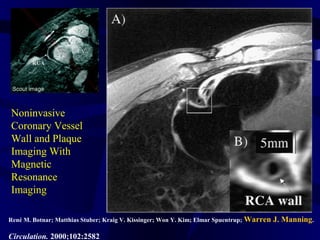
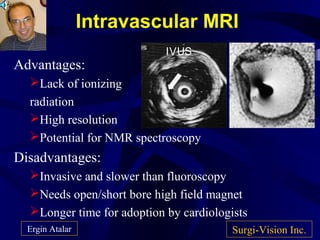
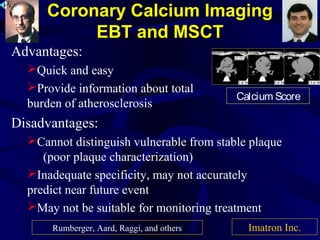







This document discusses vulnerable plaque and its role in heart attacks. It provides background on vulnerable plaque, describing it as dangerous forms of atherosclerotic plaques that can rupture or induce thrombosis. The document then reviews the history of research on vulnerable plaque, from early theories of thrombosis and inflammation to modern understanding of plaque vulnerability factors like a thin fibrous cap and large lipid core. It profiles many pioneering researchers in the field and emerging techniques for detecting vulnerable plaque, such as intravascular ultrasound, optical coherence tomography, and thermography.






















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)












