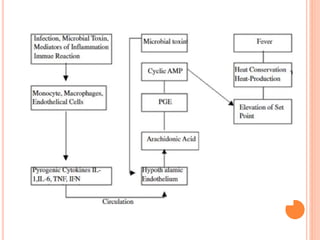
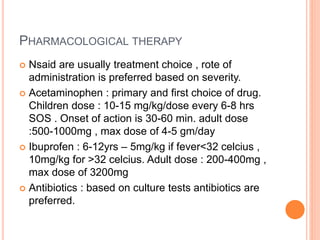
Fever is defined as a physiological condition characterized by elevated body temperature, typically over 98 to 100 degrees Fahrenheit, often associated with an underlying condition as the body works to fight off infection. There are various types of fever, including intermittent, remittent, hectic, continuous, and relapsing, with different patterns in temperature changes and potential causes ranging from infections to drug reactions. Treatment involves non-pharmacological approaches such as hydration and digestible foods, along with pharmacological methods like NSAIDs and acetaminophen for symptom relief.