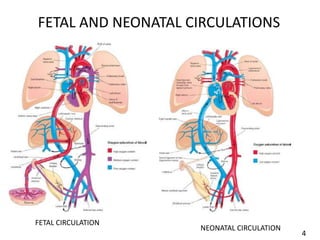
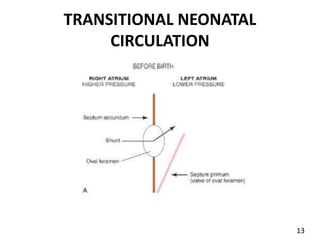
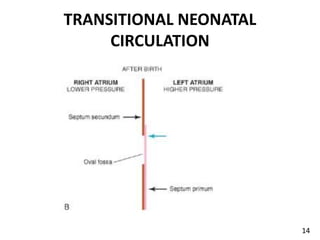
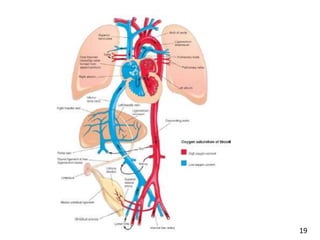
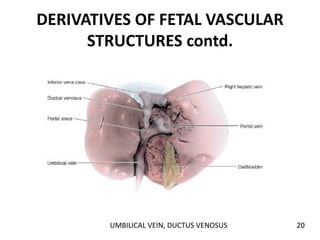
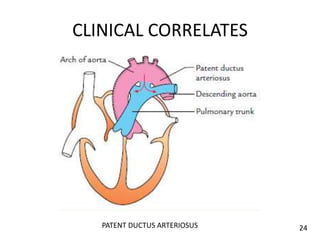
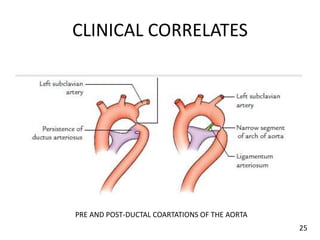
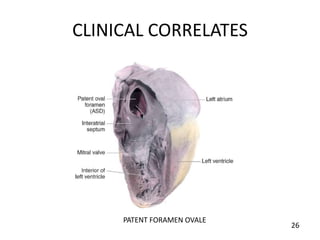
This document summarizes fetal and neonatal circulation. In the fetal circulation, oxygen-rich blood from the placenta travels to the fetus through the umbilical vein and ductus venosus, bypassing the lungs through fetal shunts. At birth, closure of the ductus venosus, foramen ovale, and ductus arteriosus occurs as the lungs become functional, establishing the neonatal circulation and excluding the placenta. Some fetal vessels like the ductus arteriosus and umbilical vessels form non-functional ligaments over time after birth.

























































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)















