Downloaded 850 times
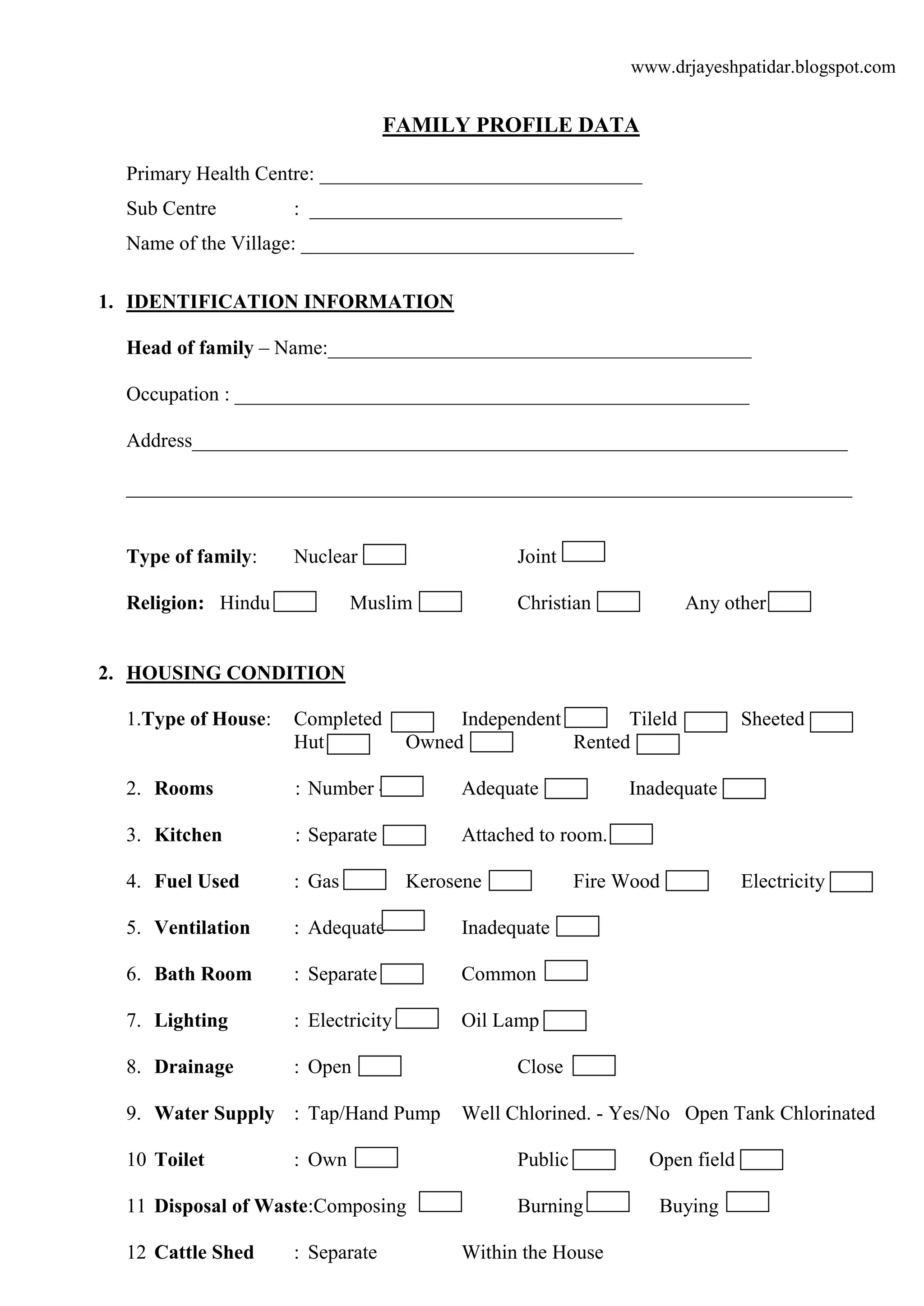
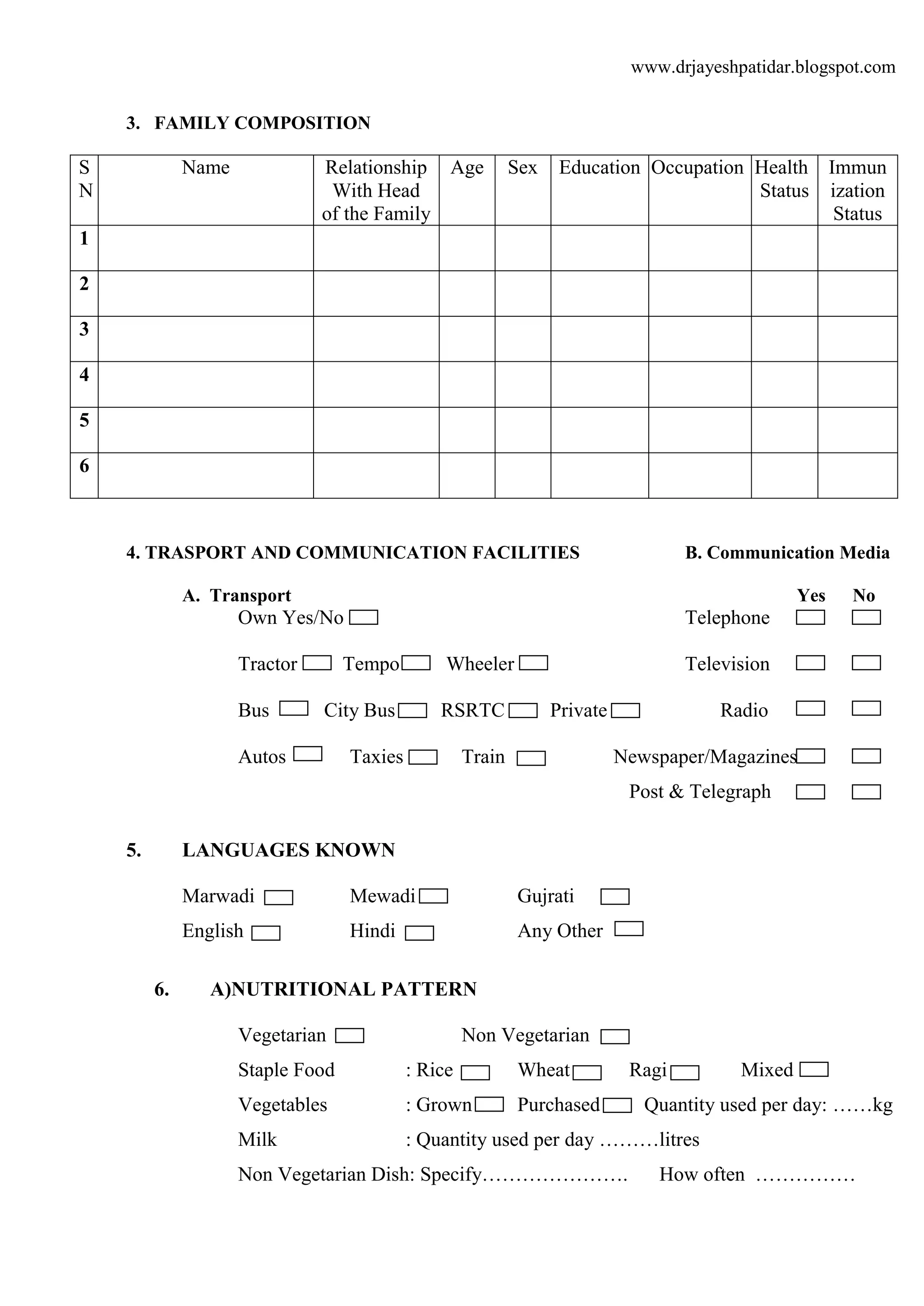
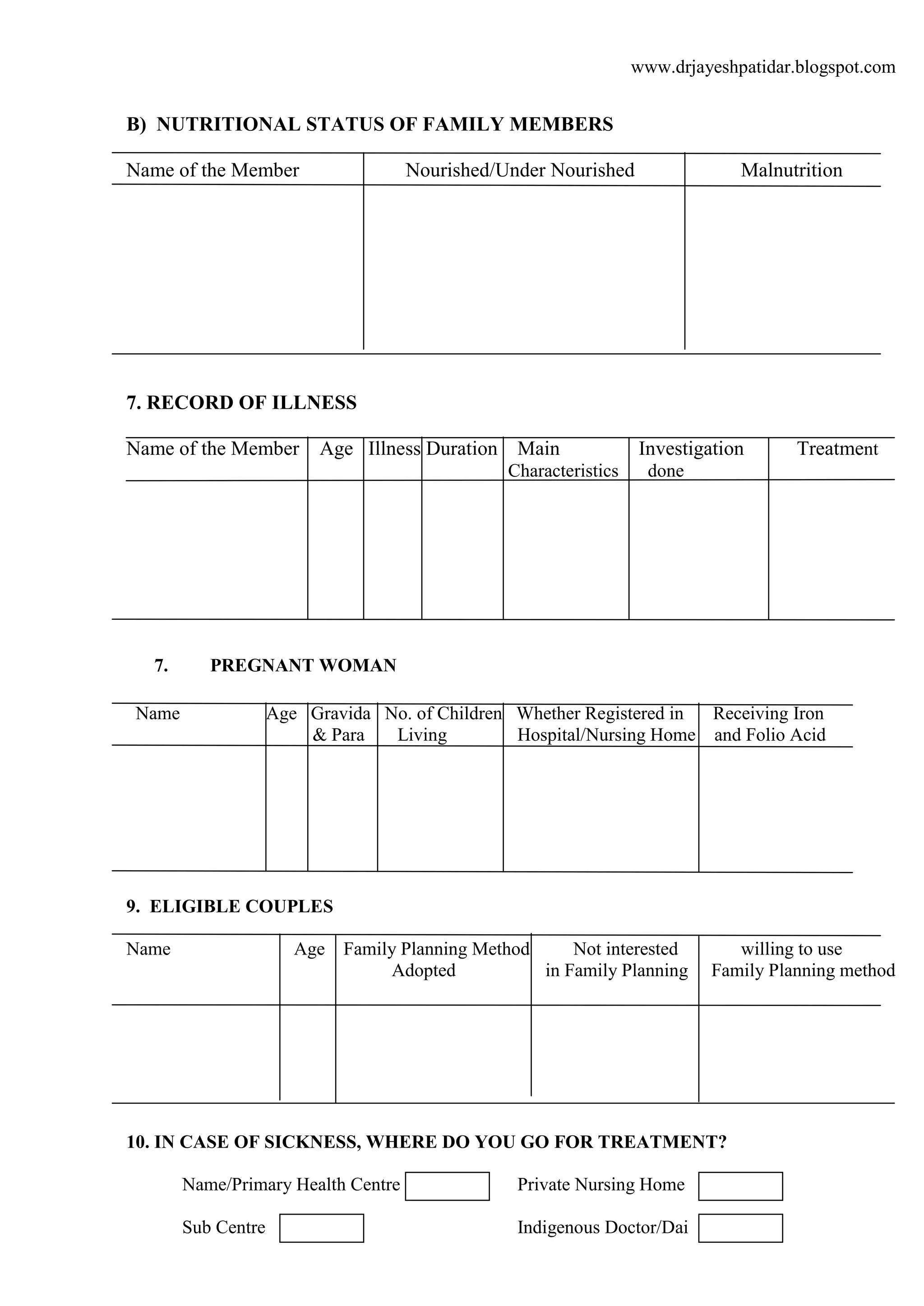
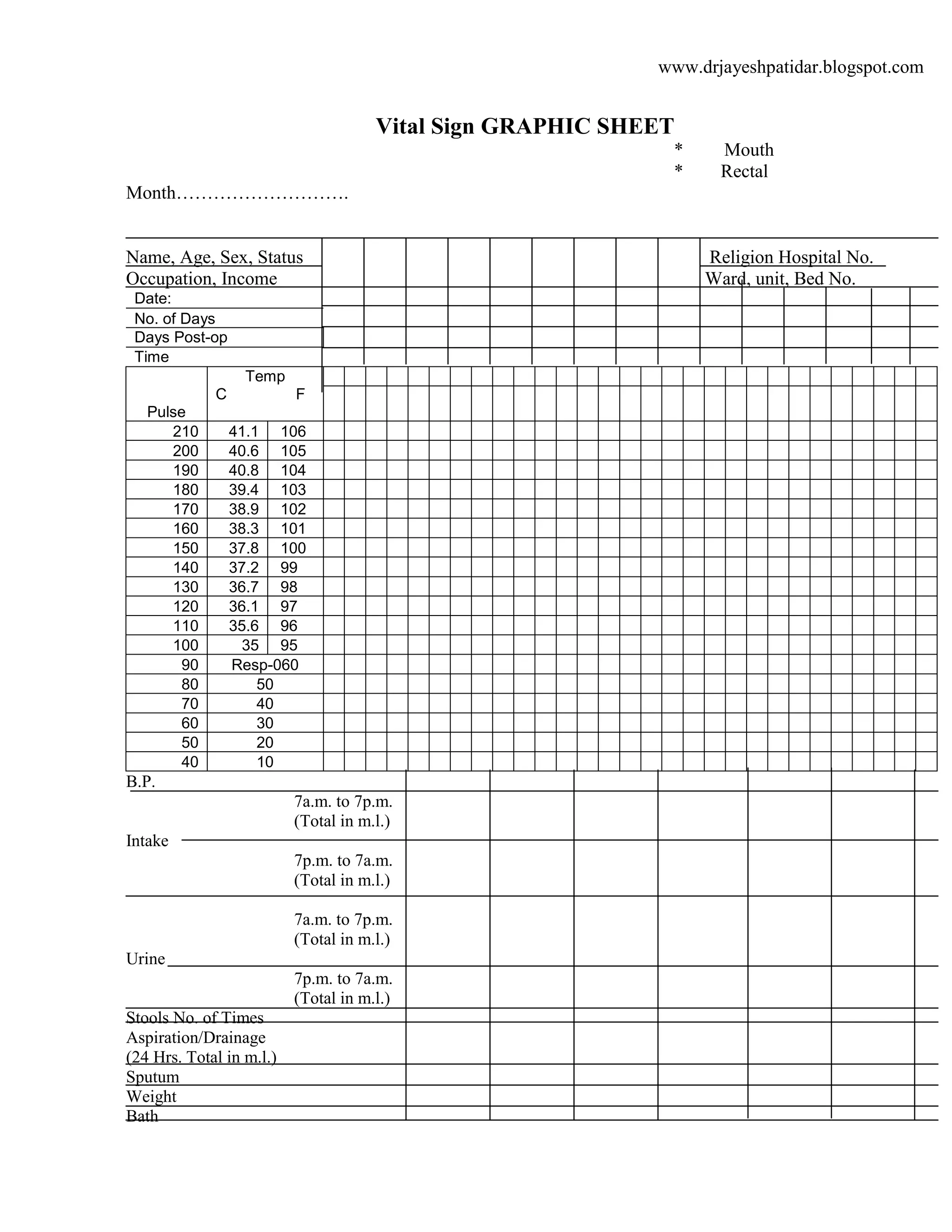

This document contains a family profile data collection form for conducting a community health nursing assessment of a family. The form collects identification information about the head of household and family members. It also gathers data on the family's housing conditions, transportation/communication access, languages spoken, nutritional patterns, health status, pregnancy/maternal health, family planning practices, and treatment seeking behavior. Nursing diagnoses, goals, interventions and outcomes are to be documented. Vital signs are to be recorded on a graphic sheet. Notes from nursing visits are also to be recorded.























































![COMMED_Sadish_Suraj1[1].pptxnnnnnnnnnnnn](https://cdn.slidesharecdn.com/ss_thumbnails/commedsadishsuraj11-241205112017-6c4912b1-thumbnail.jpg?width=640&height=640&fit=bounds)






































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)










