Downloaded 204 times







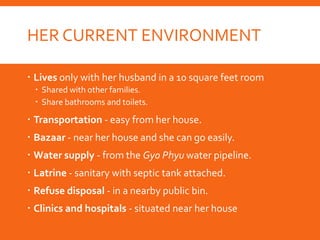
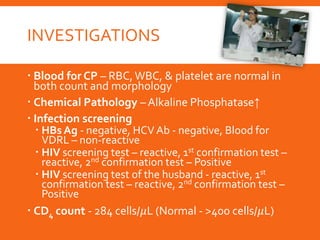


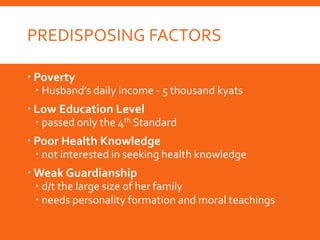









The document presents a clinico-social case of a 29-year-old female patient with HIV infection and acute gastritis, detailing her personal, social, and clinical history. Key aspects include her low income and education level, as well as the impact of her illness on family dynamics and community health. Management recommendations focus on immediate psychological support, family counseling, and long-term health education and social support measures.


























































![CBME_BATCH_2023[1].pptxCBME_BATCH_2023[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cbmebatch20231-250920121332-dd14c1c1-thumbnail.jpg?width=640&height=640&fit=bounds)





![CASE PRESENTATION prev 1 lscs[1].pptxggvvvb](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationprev1lscs1-250805135156-7e04eb55-thumbnail.jpg?width=640&height=640&fit=bounds)
![CASE PRESENTATION prev 1 lscs[1].pptxgyjgg](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationprev1lscs1-250730122151-d557d04d-thumbnail.jpg?width=640&height=640&fit=bounds)



























