Downloaded 188 times

















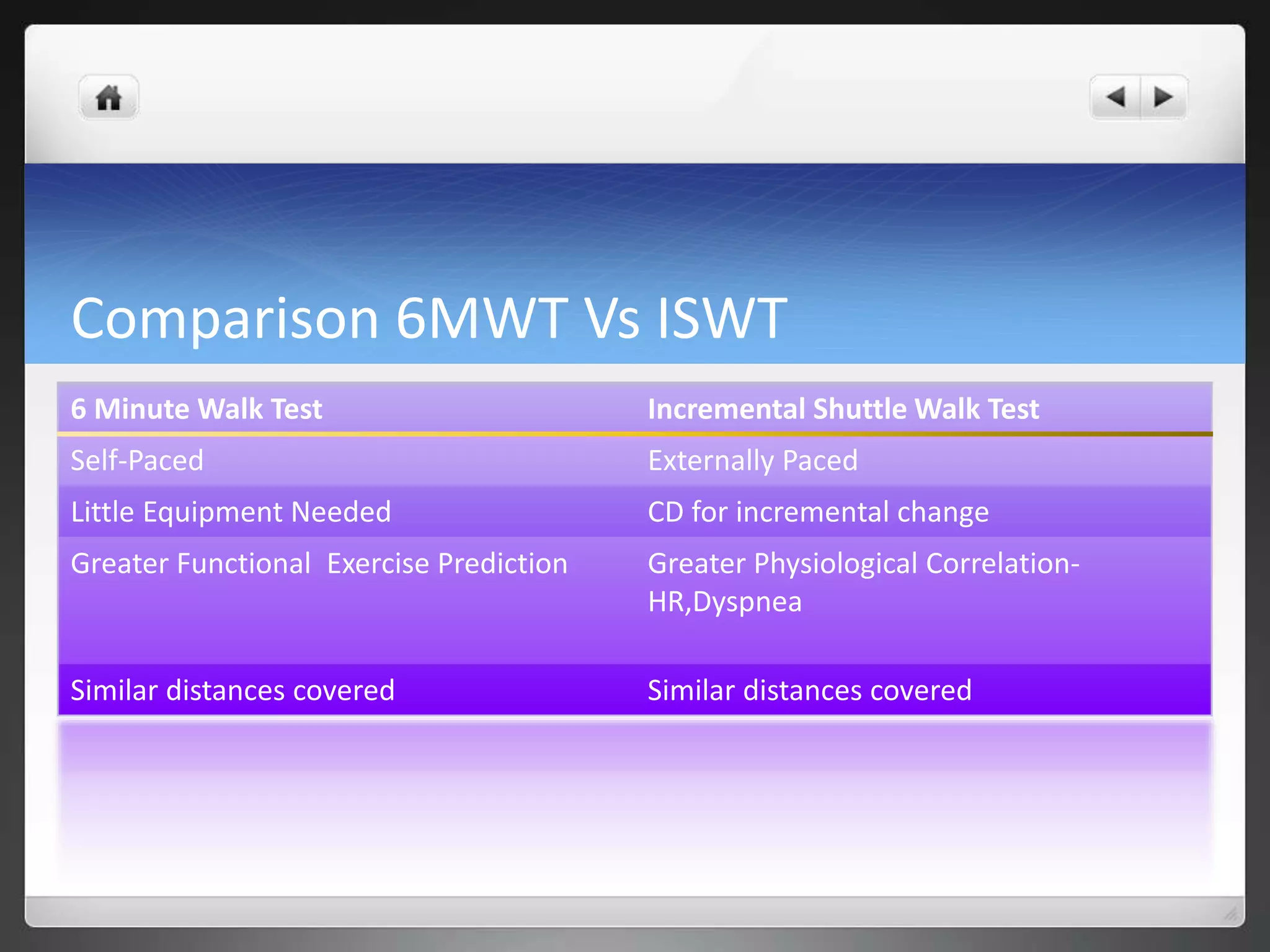





The document discusses outcome measures of functional capacity, specifically the 6-minute walk test (6MWT) and incremental shuttle walk test (ISWT). It provides background on each test, how they are implemented, evidence on their validity, reliability and responsiveness. Both tests are described as suitable measures for cardiopulmonary patients, though some evidence suggests the ISWT may better correlate to physiological measures like heart rate and dyspnea. Further research is still needed to establish the tests' validity across specific patient populations.