Downloaded 392 times

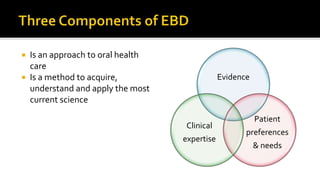

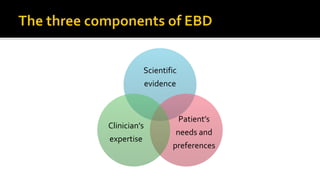
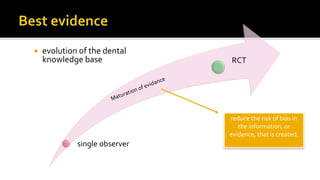



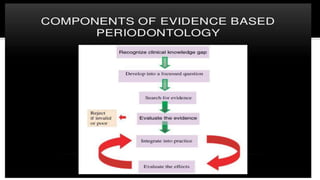
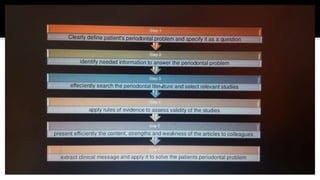

The document discusses the evolution of evidence-based dentistry (EBD), emphasizing the integration of scientific evidence, clinician expertise, and patient preferences in making clinical decisions. It highlights the development of the dental knowledge base through historical practices and the importance of systematic reviews and research methodologies like randomized controlled trials in establishing reliable treatment protocols. EBD aims to improve patient care by using the best available evidence to inform treatment decisions, fostering a more personalized approach in dental practice.



































































































