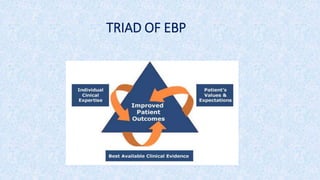
The document discusses evidence-based decision making (EBDM) in periodontics, emphasizing its importance in providing quality patient care through the integration of scientific evidence, clinical expertise, and patient preferences. It outlines the principles, advantages, and necessary skills for EBDM while comparing traditional approaches to evidence-based methods. Additionally, it highlights common barriers to implementing evidence-based dentistry among dental students and emphasizes the need for continuous learning and evaluation in clinical practice.





















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)














